

Acute effects of mixed circuit training on hemodynamic and cardiac autonomic control in chronic hemiparetic stroke patients: A randomized controlled crossover trial
- PMID: 35928565
- PMCID: PMC9343773
- DOI: 10.3389/fphys.2022.902903
Acute effects of mixed circuit training on hemodynamic and cardiac autonomic control in chronic hemiparetic stroke patients: A randomized controlled crossover trial
Abstract
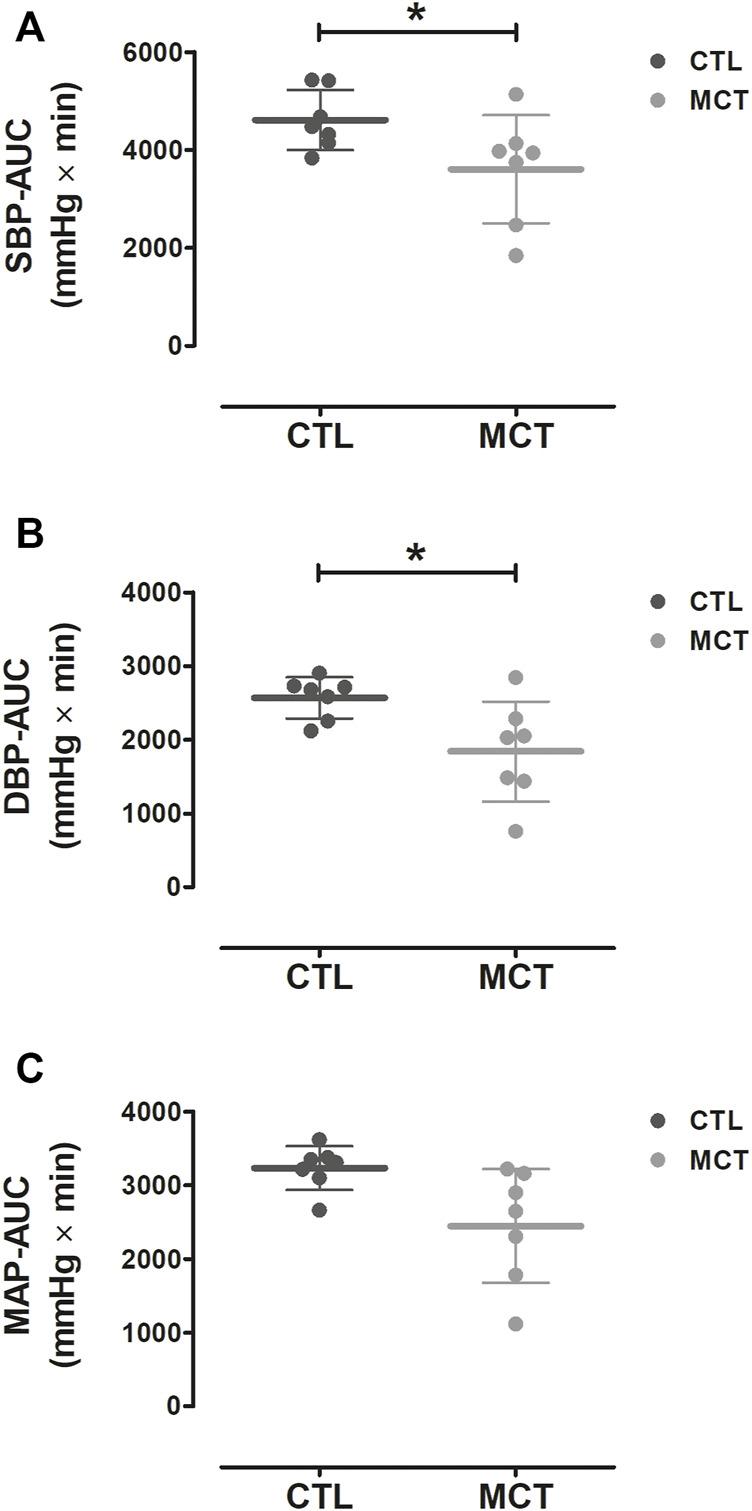
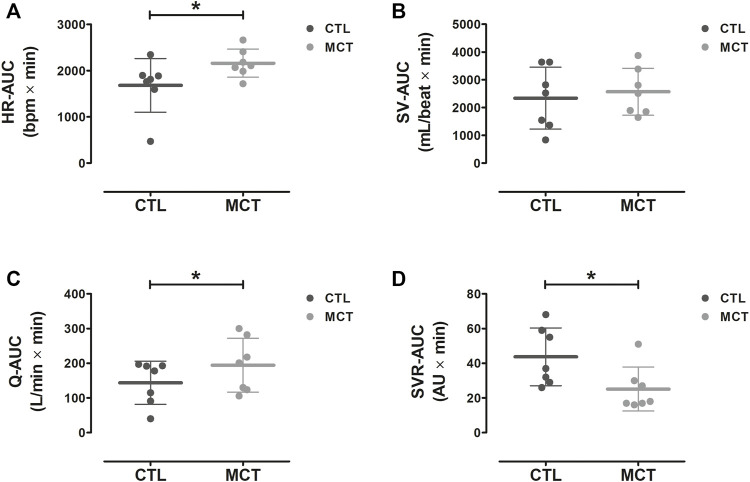
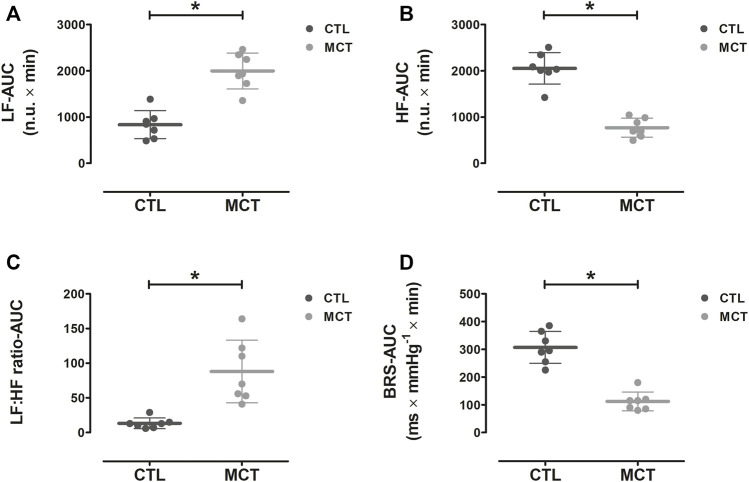
Objectives: To investigate whether a single bout of mixed circuit training (MCT) can elicit acute blood pressure (BP) reduction in chronic hemiparetic stroke patients, a phenomenon also known as post-exercise hypotension (PEH). Methods: Seven participants (58 ± 12 years) performed a non-exercise control session (CTL) and a single bout of MCT on separate days and in a randomized counterbalanced order. The MCT included 10 exercises with 3 sets of 15-repetition maximum per exercise, with each set interspersed with 45 s of walking. Systolic (SBP) and diastolic (DBP) blood pressure, mean arterial pressure (MAP), cardiac output (Q), systemic vascular resistance (SVR), baroreflex sensitivity (BRS), and heart rate variability (HRV) were assessed 10 min before and 40 min after CTL and MCT. BP and HRV were also measured during an ambulatory 24-h recovery period. Results: Compared to CTL, SBP (∆-22%), DBP (∆-28%), SVR (∆-43%), BRS (∆-63%), and parasympathetic activity (HF; high-frequency component: ∆-63%) were reduced during 40 min post-MCT (p < 0.05), while Q (∆35%), sympathetic activity (LF; low-frequency component: ∆139%) and sympathovagal balance (LF:HF ratio: ∆145%) were higher (p < 0.001). In the first 10 h of ambulatory assessment, SBP (∆-7%), MAP (∆-6%), and HF (∆-26%) remained lowered, and LF (∆11%) and LF:HF ratio (∆13%) remained elevated post-MCT vs. CTL (p < 0.05). Conclusion: A single bout of MCT elicited prolonged PEH in chronic hemiparetic stroke patients. This occurred concurrently with increased sympathovagal balance and lowered SVR, suggesting vasodilation capacity is a major determinant of PEH in these patients. This clinical trial was registered in the Brazilian Clinical Trials Registry (RBR-5dn5zd), available at https://ensaiosclinicos.gov.br/rg/RBR-5dn5zd. Clinical Trial Registration: https://ensaiosclinicos.gov.br/rg/RBR-5dn5zd, identifier RBR-5dn5zd.
Keywords: autonomic nervous system; blood pressure; circuit-based exercise; exercise; rehabilitation.
Copyright © 2022 Fonseca, Midgley, Billinger, Michalski, Costa, Monteiro, Farinatti and Cunha.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- ACSM (2013). ACSM's guidelines for exercise testing and prescription. Baltimore: Lippincott Williams & Wilkins.
-
- Anunciação P. G., Farinatti P. T., Goessler K. F., Casonatto J., Polito M. D. (2016). Blood pressure and autonomic responses following isolated and combined aerobic and resistance exercise in hypertensive older women. Clin. Exp. Hypertens. 38 (8), 710–714. 10.1080/10641963.2016.1200601 - DOI - PubMed
-
- Berg K., Wood-Dauphinee S., Williams J. (1995). The balance scale: Reliability assessment with elderly residents and patients with an acute stroke. Scand. J. Rehabil. Med. 27 (1), 27–36. - PubMed
-
- Billinger S. A., Arena R., Bernhardt J., Eng J. J., Franklin B. A., Johnson C. M., et al. (2014). Physical activity and exercise recommendations for stroke survivors: A statement for healthcare professionals from the American heart association/American stroke association. Stroke 45 (8), 2532–2553. 10.1161/STR.0000000000000022 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous