

Differences in pulmonary nodular consolidation and pulmonary cavity among drug-sensitive, rifampicin-resistant and multi-drug resistant tuberculosis patients: a computerized tomography study with history length matched cases
- PMID: 35928612
- PMCID: PMC9344412
- DOI: 10.21037/jtd-22-145
Differences in pulmonary nodular consolidation and pulmonary cavity among drug-sensitive, rifampicin-resistant and multi-drug resistant tuberculosis patients: a computerized tomography study with history length matched cases
Abstract
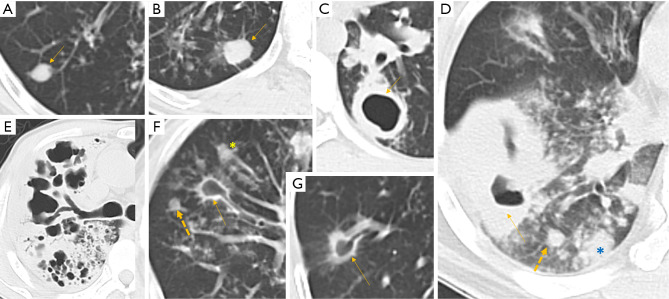
Background: There have been concerns that literature described radiological feature differences between drug-sensitive pulmonary tuberculosis (DS-PTB) and multidrug-resistant (MDR)-PTB were confounded by that MDR-PTB cases tend to have a longer history. Using history length matched DS-PTB and MDR-PTB cases from a well-defined urban region in Dalian, we retrospectively analysed the CT feature differences of these paired cases with a focus on pulmonary nodular (PN) consolidation and pulmonary cavity (PC).
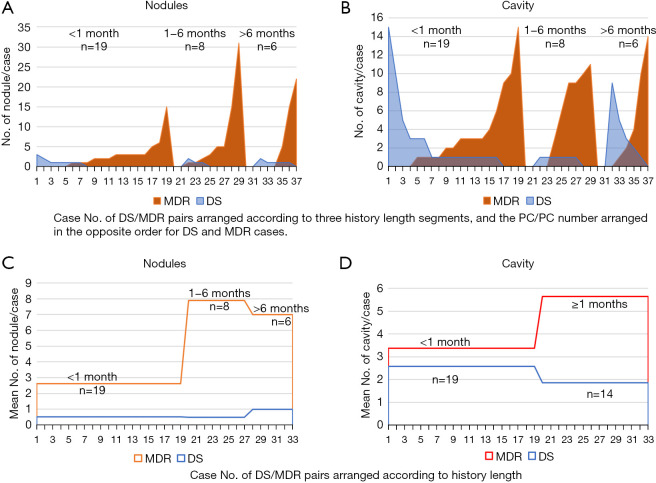
Methods: There were 33 consecutive MDR-PTB cases [inclusive of rifampicin-resistant (RR) cases, 27 males and 6 females, mean age: 49.2 years], with 19 cases had a history of <1 month and 8 and 6 cases had a history of 1-6 and >6 months respectively. To pair the MDR-PTB cases with history length, matched 33 cases of DS-PTB patients (21 males and 12 females, mean age: 56.5 years) were included. All patients were new PTB without HIV infection. The first CT exams prior to treatment were analysed.
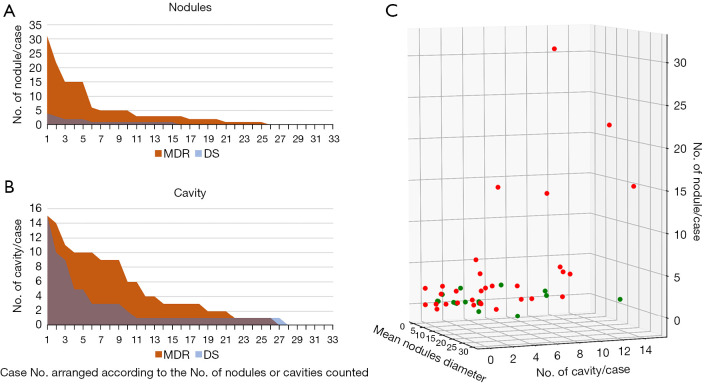
Results: Compared with DS cases, MDR cases had a much higher prevalence of PN (75.76% vs. 45.45%) and a higher number of PN per positive case for PN (6.2 vs.1.53). For the cases >1 month history, MDR-PTB had a higher number of PC per positive case than that of DS-PTB cases (7.18 vs. 2.36). To differentiate DS-PTB from MDR-PTB, receiver operating characteristic (ROC) analysis showed a cutoff PN number of ≥3 had 48.5% sensitivity and 93.9% specificity, and a cutoff PC number of ≥4 had 39.4% sensitivity and 84.9% specificity. The lung field distribution of all lesions tended to be wider for MDR-PTB cases. MDR-PTB cases appeared to be associated with a faster progression in the absence of treatment.
Conclusions: MDR-TB is likely intrinsically more invasive than DS-TB. Multiple PN and Multiple PC are promising signs for the suspicion of MDR-PTB on chest imaging.
Keywords: Differential diagnosis; computed tomography; multidrug-resistant (MDR); pulmonary; tuberculosis (TB).
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-145/coif). YXJW is the founder of Yingran Medicals Co., Ltd., which develops medical image-based diagnostics software. YXJW serves as an unpaid editorial board member of Journal of Thoracic Disease from April 2022 to March 2024. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Differences in pulmonary nodular consolidation and pulmonary cavity among drug-sensitive, rifampicin-resistant and multi-drug resistant tuberculosis patients: the Guangzhou computerized tomography study.Quant Imaging Med Surg. 2024 Jan 3;14(1):1010-1021. doi: 10.21037/qims-23-694. Epub 2023 Nov 20. Quant Imaging Med Surg. 2024. PMID: 38223080 Free PMC article.
-
Radiological signs associated with pulmonary multi-drug resistant tuberculosis: an analysis of published evidences.Quant Imaging Med Surg. 2018 Mar;8(2):161-173. doi: 10.21037/qims.2018.03.06. Quant Imaging Med Surg. 2018. PMID: 29675357 Free PMC article.
-
Chest X-ray findings in drug-sensitive and drug-resistant pulmonary tuberculosis patients in Uganda.J Clin Tuberc Other Mycobact Dis. 2022 Mar 25;27:100312. doi: 10.1016/j.jctube.2022.100312. eCollection 2022 May. J Clin Tuberc Other Mycobact Dis. 2022. PMID: 35355939 Free PMC article.
-
How We Treat Drug-Susceptible Pulmonary Tuberculosis: A Practical Guide for Clinicians.Antibiotics (Basel). 2023 Dec 14;12(12):1733. doi: 10.3390/antibiotics12121733. Antibiotics (Basel). 2023. PMID: 38136767 Free PMC article. Review.
-
Multi-modal deep learning based on multi-dimensional and multi-level temporal data can enhance the prognostic prediction for multi-drug resistant pulmonary tuberculosis patients.Sci One Health. 2022 Nov 23;1:100004. doi: 10.1016/j.soh.2022.100004. eCollection 2022 Nov. Sci One Health. 2022. PMID: 39076608 Free PMC article. Review.
Cited by
-
Chinese expert consensus on imaging diagnosis of drug-resistant pulmonary tuberculosis.Quant Imaging Med Surg. 2024 Jan 3;14(1):1039-1060. doi: 10.21037/qims-23-1223. Epub 2023 Oct 25. Quant Imaging Med Surg. 2024. PMID: 38223121 Free PMC article. Review.
-
Computed Tomography Manifestations in Patients with Rifampin Primary Drug-Resistant Tuberculosis in an Infectious Disease Hospital in the Yi Autonomous Prefecture, China.Int J Gen Med. 2023 Nov 6;16:5109-5118. doi: 10.2147/IJGM.S428962. eCollection 2023. Int J Gen Med. 2023. PMID: 37954652 Free PMC article.
-
Deep learning for precise diagnosis and subtype triage of drug-resistant tuberculosis on chest computed tomography.MedComm (2020). 2024 Mar 10;5(3):e487. doi: 10.1002/mco2.487. eCollection 2024 Mar. MedComm (2020). 2024. PMID: 38469547 Free PMC article.
-
Differences in pulmonary nodular consolidation and pulmonary cavity among drug-sensitive, rifampicin-resistant and multi-drug resistant tuberculosis patients: the Guangzhou computerized tomography study.Quant Imaging Med Surg. 2024 Jan 3;14(1):1010-1021. doi: 10.21037/qims-23-694. Epub 2023 Nov 20. Quant Imaging Med Surg. 2024. PMID: 38223080 Free PMC article.
References
-
- World Health Organization. Global Tuberculosis Report 2019. Available online: https://www.who.int/publications/i/item/9789241565714
LinkOut - more resources
Full Text Sources