

Efficacy of low-dose corticosteroids in patients with acute respiratory distress syndrome: a prospective observational study
- PMID: 35928619
- PMCID: PMC9344422
- DOI: 10.21037/jtd-21-890
Efficacy of low-dose corticosteroids in patients with acute respiratory distress syndrome: a prospective observational study
Abstract
Background: There is still no agreement on whether corticosteroids can reduce mortality in patients with acute respiratory distress syndrome (ARDS). The aim of this study was to investigate the efficacy of low-dose corticosteroid administration in patients with ARDS.
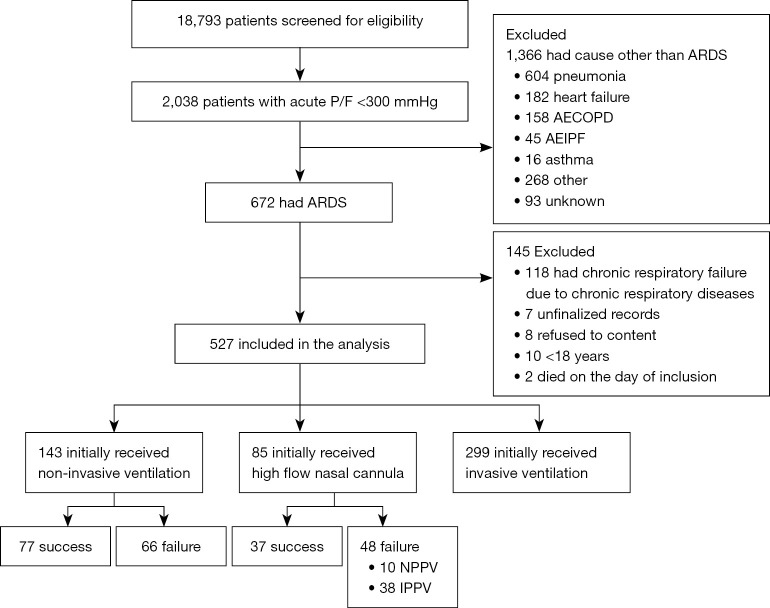
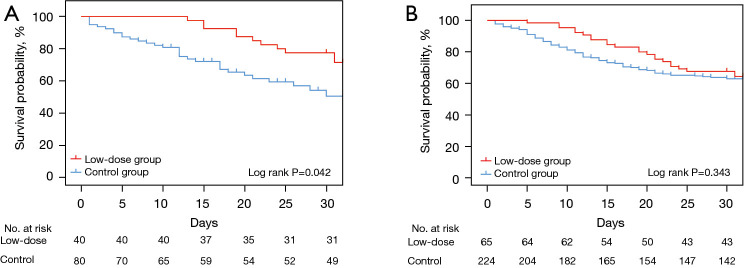
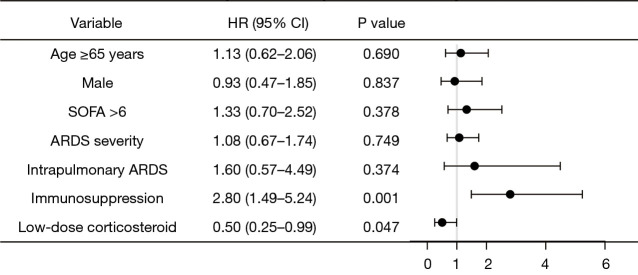
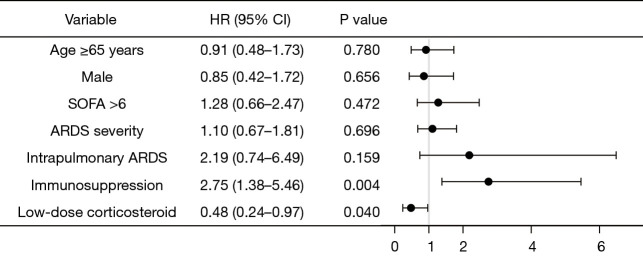
Methods: A prospective observational study of patients with ARDS in 17 hospitals in China was performed between March 2016 and February 2018. Propensity score matching was performed to adjust for differences in baseline characteristics between different groups. The effects of corticosteroids were assessed by using the Kaplan-Meier method and a multivariate Cox regression.
Results: A total of 527 ARDS patients were enrolled in the study. Sixty-five patients (12.3%) were administered low-dose (methylprednisolone ≤1 mg·kg-1·d-1) corticosteroids. The median dose was equivalent to 0.67 (0.57-0.81) mg/kg methylprednisolone for a median duration of 10 days. The control group included 224 patients (42.5%) who had never receive corticosteroids. In the matched sample, the hospital mortality rates in the low-dose (n=40) and control groups (n=80) were 27.5% and 42.5% (P=0.110), respectively. The length of hospital stay was significantly longer in the low-dose corticosteroid group than in the control group (24.0 vs. 17.0, P=0.002), and the multivariate Cox regression analysis suggested that the low-dose group had a significantly lower risk of death than the control group (HR: 0.48; 95% CI: 0.24-0.97; P=0.040).
Conclusions: The administration of low-dose corticosteroids may reduce mortality in patients with ARDS.
Keywords: Acute respiratory distress syndrome (ARDS); corticosteroid; mortality.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-21-890/coif). All authors report funding from Beijing Municipal Science & Technology Commission, National Natural Science Foundation, and Chinese Academy of Medical Sciences.
Figures
References
-
- ARDS Definition Task Force ; Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA 2012;307:2526-33. - PubMed
LinkOut - more resources
Full Text Sources