

Femoral Shaft Fracture in Post-polio Syndrome Patients: Case Series from a Level-I Trauma Center and Review of Literature
- PMID: 35928657
- PMCID: PMC9283591
- DOI: 10.1007/s43465-022-00683-8
Femoral Shaft Fracture in Post-polio Syndrome Patients: Case Series from a Level-I Trauma Center and Review of Literature
Erratum in
-
Correction to: Femoral Shaft Fracture in Post-polio Syndrome Patients: Case Series from a Level-I Trauma Center and Review of Literature.Indian J Orthop. 2022 Nov 29;57(1):166. doi: 10.1007/s43465-022-00764-8. eCollection 2023 Jan. Indian J Orthop. 2022. PMID: 36660491 Free PMC article.
Abstract
Background: Femoral shaft fracture in patients of post-polio syndrome (PPS) represents an uncommon yet complex injury pattern. Poorly developed soft-tissue envelope, decreased muscle bulk, reduced vascularity, regional osteopenia, joint contractures, and altered bony anatomy impose significant surgical challenges. Thorough pre-operative planning is imperative as each case requires individualized approach and method of fixation. The aim of the study was to analyze the clinical outcomes in such patients following fracture fixation and to assess the surgical challenges encountered and provide solutions.
Materials and methods: A retrospective case series of 33 patients with femoral shaft fracture in PPS limbs was undertaken. Mode of injury, method of fixation, surgical time, intra-operative blood loss, union time, and complications were recorded.
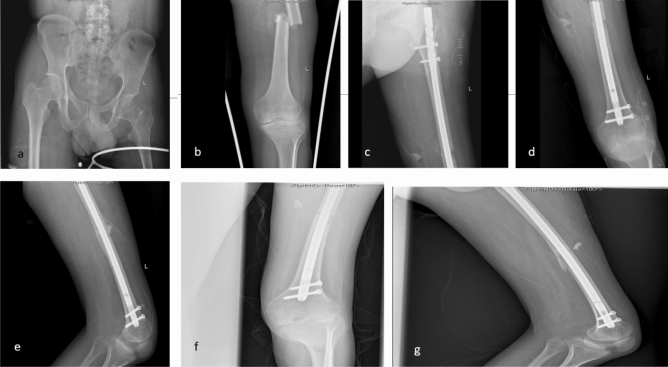
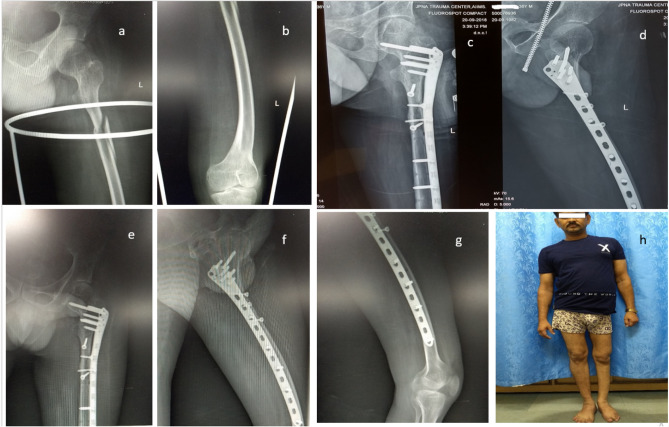
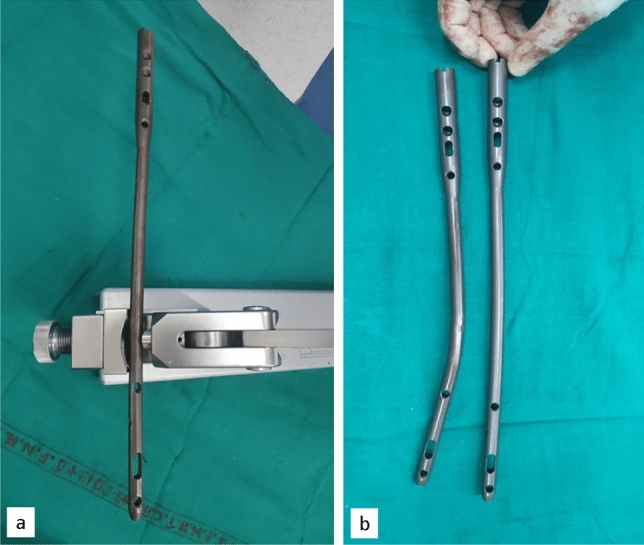
Results: Low-energy fall was the most common mechanism of injury (73%). Thirty-three patients underwent fixation with intramedullary nailing being the most common mode (79%). Femoral canal diameter, femoral bow, fracture location and morphology and clinical deformities of the patients are key governing factors that determine the choice of implant. Locking plates, pre-contoured anatomical plates, and titanium elastic nailing system offer an alternative in patients unsuitable for nailing. With no difference between various implants, average time for bone healing was 13.8 ± 4.4 weeks. All patients resumed full weight-bearing mobilization and returned to pre-injury activity status at the end of 6 months post-surgery.
Conclusion: With detailed pre-operative work-up, contemplating intra-operative difficulties, individualized surgical plan, careful handling of soft tissues, and availability of back-up implants, good clinical outcomes can be achieved in femur fractures in PPS patients.
Keywords: Femur shaft fracture; Intramedullary nailing; PPS; Post-polio syndrome.
© Indian Orthopaedics Association 2022.
Conflict of interest statement
Conflict of InterestThe authors (Suman Saurabh, Anupam Gupta, Tanya Trikha, Aashraya Karpe, and Samarth Mittal) declare that they have no conflict of interests. Authors also declare that no funding has been received from any source.
Figures


Similar articles
-
Ipsilateral femoral neck and shaft fractures: case series from a single Level-I trauma centre and review of literature.Eur J Orthop Surg Traumatol. 2023 May;33(4):803-809. doi: 10.1007/s00590-021-03199-3. Epub 2022 Feb 4. Eur J Orthop Surg Traumatol. 2023. PMID: 35119486 Review.
-
Elastic Stable Titanium Flexible Intramedullary Nails Versus Plates in Treating Low Grade Comminuted Femur Shaft Fractures in Children.Orthop Surg. 2019 Aug;11(4):664-670. doi: 10.1111/os.12514. Orthop Surg. 2019. PMID: 31456324 Free PMC article.
-
Elastic stable intramedullary nailing (ESIN) in paediatric femur and tibia shaft fractures: Comparison between titanium and stainless steel nails.Injury. 2018 Nov;49 Suppl 3:S8-S11. doi: 10.1016/j.injury.2018.09.049. Injury. 2018. PMID: 30415674
-
Conversion of external fixation to intramedullary nailing for fractures of the shaft of the femur in multiply injured patients.J Bone Joint Surg Am. 2000 Jun;82(6):781-8. J Bone Joint Surg Am. 2000. PMID: 10859097
-
Management Options and Outcomes for Patients with Femoral Fractures with Post-Polio Syndrome of the Lower Extremity: A Critical Analysis Review.JBJS Rev. 2020 Jun;8(6):e0146. doi: 10.2106/JBJS.RVW.19.00146. JBJS Rev. 2020. PMID: 32487976 Review.
Cited by
-
Tailoring the approach: Management of femur fractures in post-polio syndrome patients.J Clin Orthop Trauma. 2025 Mar 17;65:102979. doi: 10.1016/j.jcot.2025.102979. eCollection 2025 Jun. J Clin Orthop Trauma. 2025. PMID: 40213504
-
Reconstructing the Gait Pattern of a Korean Cadaver with Bilateral Lower Limb Asymmetry Using a Virtual Humanoid Modeling Program.Diagnostics (Basel). 2025 Aug 2;15(15):1943. doi: 10.3390/diagnostics15151943. Diagnostics (Basel). 2025. PMID: 40804908 Free PMC article.
-
Peri-implant proximal femur fracture in a poliomyelitis survivor: A surgical and medical challenge.Clin Case Rep. 2023 Jun 5;11(6):e7465. doi: 10.1002/ccr3.7465. eCollection 2023 Jun. Clin Case Rep. 2023. PMID: 37287621 Free PMC article.
References
-
- Poliomyelitis (polio) [Internet]. [cited 2021 Jun 26]. https://www.who.int/westernpacific/health-topics/poliomyelitis. Accessed 26 June 2021
LinkOut - more resources
Full Text Sources