

Case Report: Progression of a Silent Corticotroph Tumor to an Aggressive Secreting Corticotroph Tumor, Treated by Temozolomide. Changes in the Clinic, the Pathology, and the β-Catenin and α-SMA Expression
- PMID: 35928898
- PMCID: PMC9344046
- DOI: 10.3389/fendo.2022.870172
Case Report: Progression of a Silent Corticotroph Tumor to an Aggressive Secreting Corticotroph Tumor, Treated by Temozolomide. Changes in the Clinic, the Pathology, and the β-Catenin and α-SMA Expression
Abstract
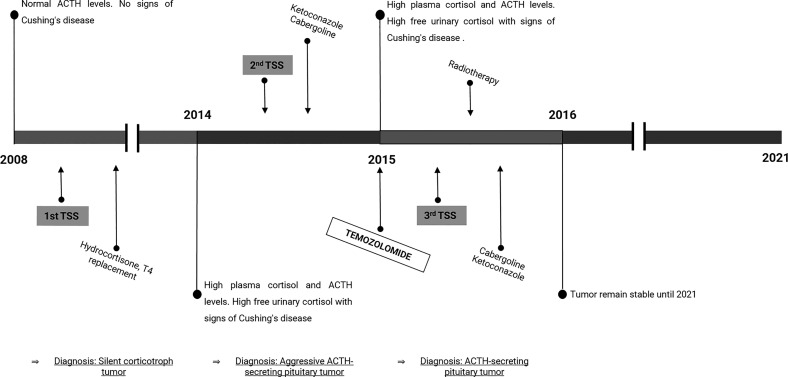
Clinically silent corticotroph tumors are usually macroadenomas that comprise 20% of ACTH tumors. They frequently progress to aggressive tumors with high recurrence, invasiveness, and on rare occasions, they may become hormonally active causing Cushing's disease. Trustable biomarkers that can predict their aggressive course, as well as their response to traditional or new therapies, are paramount. Aberrant β-Catenin expression and localization have been proposed as responsible for several malignancies including pituitary tumors. Nevertheless, the role of β-Catenin in the aggressive transformation of silent corticotropinomas and their response to Temozolomide salvage treatment have not been explored yet. In this work, we present a case of a silent corticotroph tumor that invaded cavernous sinus and compressed optic chiasm and, after a first total resection and tumor remission it recurred six years later as an aggressive ACTH-secreting tumor. This lesion grew with carotid compromise and caused Cushing's signs. It required multiple medical treatments including Cabergoline, Ketoconazole, TMZ, and radiotherapy. Besides, other two surgeries were needed until it could be controlled. Interestingly, we found α-SMA vascular area reduction and differential β-Catenin cell localization in the more aggressive tumor stages characterized by high Ki-67 indexes and p53 expression. Our results may indicate a role of angiogenesis and β-Catenin trigged events in the pituitary tumor progression, which could in turn affect the response to TMZ and/or conventional treatments. These molecular findings in this unusual case could be useful for future management of aggressive pituitary tumors.
Keywords: ACTH; corticotroph tumor; temozolomide; tumor transformation; vasculature; β-Catenin.
Copyright © 2022 Demarchi, Perrone, Esper Romero, De Bonis, Casasco, Sevlever, Berner and Cristina.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Aggressive Cushing's Disease: Molecular Pathology and Its Therapeutic Approach.Front Endocrinol (Lausanne). 2021 Jun 16;12:650791. doi: 10.3389/fendo.2021.650791. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34220707 Free PMC article. Review.
-
The expression of glucocorticoid and mineralocorticoid receptors in pituitary tumors causing Cushing's disease and silent corticotroph tumors.Front Endocrinol (Lausanne). 2023 Mar 29;14:1124646. doi: 10.3389/fendo.2023.1124646. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37065760 Free PMC article.
-
Clinical, Laboratory, and Treatment Profiles of Silent Corticotroph Adenomas That Have Transformed to the Functional Type: A Case Series With a Literature Review.Front Endocrinol (Lausanne). 2020 Sep 23;11:558593. doi: 10.3389/fendo.2020.558593. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 33071973 Free PMC article.
-
Successful reduction of ACTH secretion in a case of intractable Cushing's disease with pituitary Crooke's cell adenoma by combined modality therapy including temozolomide.Endocr J. 2019 Aug 29;66(8):701-708. doi: 10.1507/endocrj.EJ18-0547. Epub 2019 May 25. Endocr J. 2019. PMID: 31130573
-
Aggressive corticotroph tumors and carcinomas.J Neuroendocrinol. 2022 Aug;34(8):e13169. doi: 10.1111/jne.13169. Epub 2022 Aug 18. J Neuroendocrinol. 2022. PMID: 35979732 Free PMC article. Review.
Cited by
-
Phenotype Transformation of PitNETs.Cancers (Basel). 2024 Apr 29;16(9):1731. doi: 10.3390/cancers16091731. Cancers (Basel). 2024. PMID: 38730682 Free PMC article. Review.
-
Research progress on the role of the Wnt signaling pathway in pituitary adenoma.Front Endocrinol (Lausanne). 2023 Sep 14;14:1216817. doi: 10.3389/fendo.2023.1216817. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37780610 Free PMC article. Review.
References
-
- Young WF. Clinically Nonfunctioning Pituitary Adenomas. In: Thapar K, Kovacs K, Scheithauer BW, Lloyd RV, editors. Diagnosis and Management of Pituitary Tumors. Totowa, NJ: Humana Press; (2001). p. 343–51.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous