

Posteriorly Displaced Radial Head Fractures May Represent the Footprint of an Elbow Dislocation or Subluxation as a Variant of Modified Mason Type 4
- PMID: 35928906
- PMCID: PMC9295585
- DOI: 10.22038/ABJS.2021.55486.2764
Posteriorly Displaced Radial Head Fractures May Represent the Footprint of an Elbow Dislocation or Subluxation as a Variant of Modified Mason Type 4
Abstract
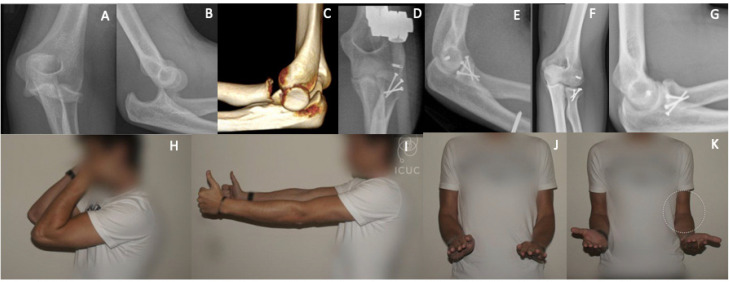
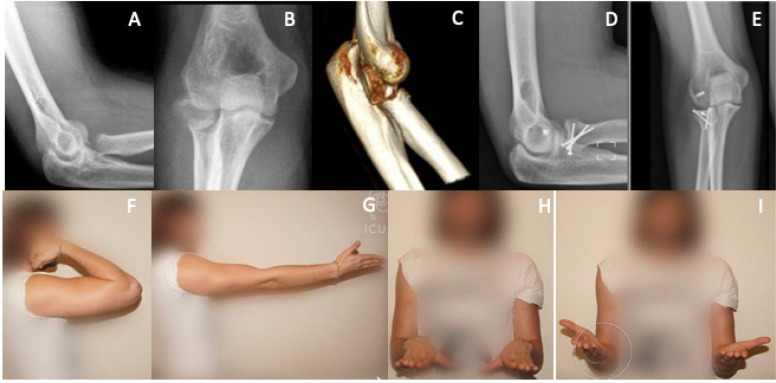
Background: The purpose of this case series is to describe surgical decision making and clinical outcomes in posteriorly displaced radial head fractures with a major fragment (more than 50% of the head) located behind the humeral condyle. We also document the outcome of open reduction and internal fixation of completely displaced radial head fractures.
Methods: A retrospective review of the ICUC® (Integrated Comprehensive Unchanged Complete) database was performed between 2012 and 2020. Patients were included if preoperative radiographs demonstrated a major radial head fracture fragment located posterior to the humeral condyle and a minimum of 2-year follow-up data was available.
Results: Ten patients met inclusion criteria. Two patients had an associated elbow dislocation whereas 8 patients did not. All patients were found to have disruption of the lateral collateral ligament complex intraoperatively. Nine radial head fractures were successfully fixed with interfragmentary screws. One multi-fragmented radial head fracture could not be successfully stabilized with interfragmentary screw fixation and was resected. The average time to final follow-up was 4.8 years (range 2.2-8.1). At final follow-up, 6 patients demonstrated radiographic evidence of a healed radial head, 1 patient had avascular necrosis, and 2 had post-traumatic arthritis. None demonstrated radiographic instability. The average functional score was 0.64 (SD 0.81) and pain score was 0.45 (SD 0.93). The average elbow extension was 8 degrees (SD 11), elbow flexion was 139 degrees (SD 6), forearm supination was 60 degrees (SD 27), and forearm pronation was 69 degrees (SD 3).
Conclusion: Recognition of a posteriorly displaced radial head fracture is essential, as it may be an indirect sign of elbow instability. This instability should be addressed during surgical intervention.
Keywords: Elbow; Elbow dislocation; Radial head fracture; Trauma.
Figures
References
-
- Beingessner DM, Dunning CE, Gordon KD, Johnson JA, King GJW. The effect of radial head fracture size on elbow kinematics and stability. J Orthop Res off Publ Orthop Res Soc. 2005;23(1):210–7. - PubMed
-
- Rineer CA, Guitton TG, Ring D. Radial head fractures: loss of cortical contact is associated with concomitant fracture or dislocation. J Shoulder Elbow Surg. 2010;19(1):21–5. - PubMed
-
- Regazzoni P, Giannoudis PV, Lambert S, Fernandez A, Perren SM. The ICUC® app: Can it pave the way for quality control and transparency in medicine? Injury. 2017;48(6):1101–3. - PubMed
-
- Regazzoni P, Südkamp N, Fernandez A, Perren SM. A new way to learn and analyze surgical interventions. Orthopedics and Trauma Surgery messages and news. 2016
LinkOut - more resources
Full Text Sources
Miscellaneous