

Ablation and antiarrhythmic drug effects on PITX2 +/- deficient atrial fibrillation: A computational modeling study
- PMID: 35928934
- PMCID: PMC9343754
- DOI: 10.3389/fcvm.2022.942998
Ablation and antiarrhythmic drug effects on PITX2 +/- deficient atrial fibrillation: A computational modeling study
Abstract
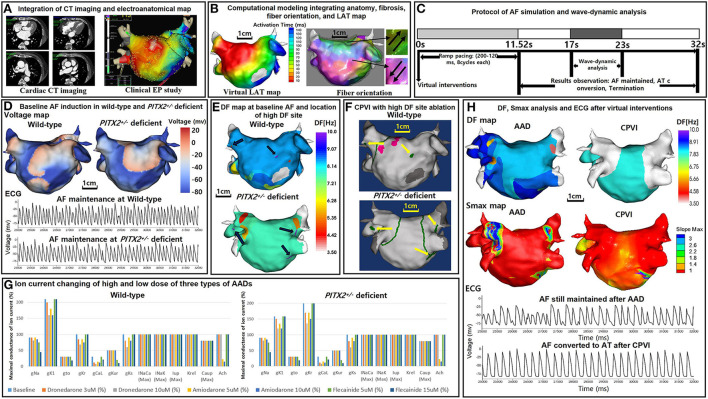
Introduction: Atrial fibrillation (AF) is a heritable disease, and the paired-like homeodomain transcription factor 2 (PITX2) gene is highly associated with AF. We explored the differences in the circumferential pulmonary vein isolation (CPVI), which is the cornerstone procedure for AF catheter ablation, additional high dominant frequency (DF) site ablation, and antiarrhythmic drug (AAD) effects according to the patient genotype (wild-type and PITX2 +/- deficient) using computational modeling.
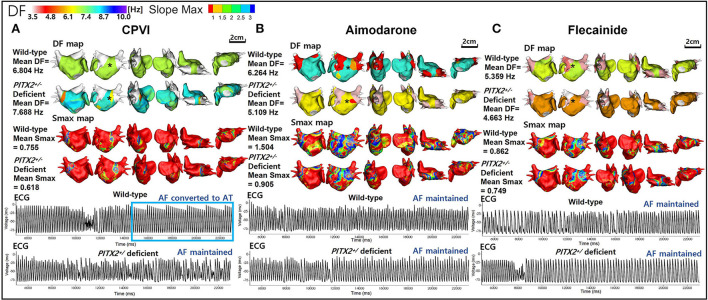
Methods: We included 25 patients with AF (68% men, 59.8 ± 9.8 years of age, 32% paroxysmal AF) who underwent AF catheter ablation to develop a realistic computational AF model. The ion currents for baseline AF and the amiodarone, dronedarone, and flecainide AADs according to the patient genotype (wild type and PITX2 +/- deficient) were defined by relevant publications. We tested the virtual CPVI (V-CPVI) with and without DF ablation (±DFA) and three virtual AADs (V-AADs, amiodarone, dronedarone, and flecainide) and evaluated the AF defragmentation rates (AF termination or changes to regular atrial tachycardia (AT), DF, and maximal slope of the action potential duration restitution curves (Smax), which indicates the vulnerability of wave-breaks.
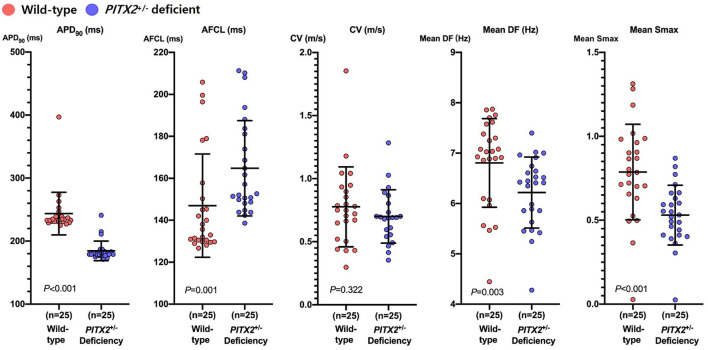
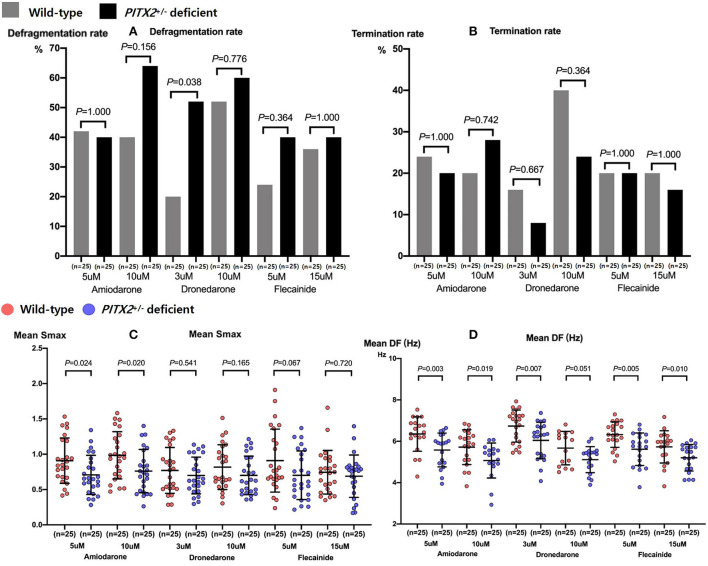
Results: At the baseline AF, mean DF (p = 0.003), and Smax (p < 0.001) were significantly lower in PITX2 +/- deficient patients than wild-type patients. In the overall AF episodes, V-CPVI (±DFA) resulted in a higher AF defragmentation relative to V-AADs (65 vs. 42%, p < 0.001) without changing the DF or Smax. Although a PITX2 +/- deficiency did not affect the AF defragmentation rate after the V-CPVI (±DFA), V-AADs had a higher AF defragmentation rate (p = 0.014), lower DF (p < 0.001), and lower Smax (p = 0.001) in PITX2 +/- deficient AF than in wild-type patients. In the clinical setting, the PITX2 +/- genetic risk score did not affect the AF ablation rhythm outcome (Log-rank p = 0.273).
Conclusion: Consistent with previous clinical studies, the V-CPVI had effective anti-AF effects regardless of the PITX2 genotype, whereas V-AADs exhibited more significant defragmentation or wave-dynamic change in the PITX2 +/- deficient patients.
Keywords: PITX2; antiarrhythmic drug; atrial fibrillation; computational modeling; dominant frequency.
Copyright © 2022 Jin, Hwang, Lim, Kwon, Park, Yu, Kim, Joung, Lee and Pak.
Figures
Similar articles
-
Computational Modeling for Antiarrhythmic Drugs for Atrial Fibrillation According to Genotype.Front Physiol. 2021 May 13;12:650449. doi: 10.3389/fphys.2021.650449. eCollection 2021. Front Physiol. 2021. PMID: 34054570 Free PMC article.
-
Spatial Changes in the Atrial Fibrillation Wave-Dynamics After Using Antiarrhythmic Drugs: A Computational Modeling Study.Front Physiol. 2021 Sep 24;12:733543. doi: 10.3389/fphys.2021.733543. eCollection 2021. Front Physiol. 2021. PMID: 34630153 Free PMC article.
-
Anti-atrial Fibrillation Effects of Pulmonary Vein Isolation With or Without Ablation Gaps: A Computational Modeling Study.Front Physiol. 2022 Mar 17;13:846620. doi: 10.3389/fphys.2022.846620. eCollection 2022. Front Physiol. 2022. PMID: 35370797 Free PMC article.
-
Antiarrhythmic drugs for atrial fibrillation: lessons from the past and opportunities for the future.Europace. 2021 Apr 10;23(23 Suppl 2):ii14-ii22. doi: 10.1093/europace/euaa426. Europace. 2021. PMID: 33837753 Review.
-
Long-Term Outcomes and Improvements in Quality of Life in Patients with Atrial Fibrillation Treated with Catheter Ablation vs. Antiarrhythmic Drugs.Am J Cardiovasc Drugs. 2021 May;21(3):299-320. doi: 10.1007/s40256-020-00435-9. Am J Cardiovasc Drugs. 2021. PMID: 33000397
Cited by
-
Clinical usefulness of digital twin guided virtual amiodarone test in patients with atrial fibrillation ablation.NPJ Digit Med. 2024 Oct 23;7(1):297. doi: 10.1038/s41746-024-01298-z. NPJ Digit Med. 2024. PMID: 39443659 Free PMC article.
-
Digital Twin Models in Atrial Fibrillation: Charting the Future of Precision Therapy?J Pers Med. 2025 Jun 16;15(6):256. doi: 10.3390/jpm15060256. J Pers Med. 2025. PMID: 40559118 Free PMC article. Review.
-
What determines the optimal pharmacological treatment of atrial fibrillation? Insights from in silico trials in 800 virtual atria.J Physiol. 2023 Sep;601(18):4013-4032. doi: 10.1113/JP284730. Epub 2023 Jul 20. J Physiol. 2023. PMID: 37475475 Free PMC article.
References
-
- Kim D, Yang PS, Jang E, Yu HT, Kim TH, Uhm JS, et al. . 10-Year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am Heart J. (2018) 202:20–6. 10.1016/j.ahj.2018.04.017 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous