

Development and Validation of a Personalized, Sex-Specific Prediction Algorithm of Severe Atheromatosis in Middle-Aged Asymptomatic Individuals: The ILERVAS Study
- PMID: 35928938
- PMCID: PMC9344070
- DOI: 10.3389/fcvm.2022.895917
Development and Validation of a Personalized, Sex-Specific Prediction Algorithm of Severe Atheromatosis in Middle-Aged Asymptomatic Individuals: The ILERVAS Study
Abstract
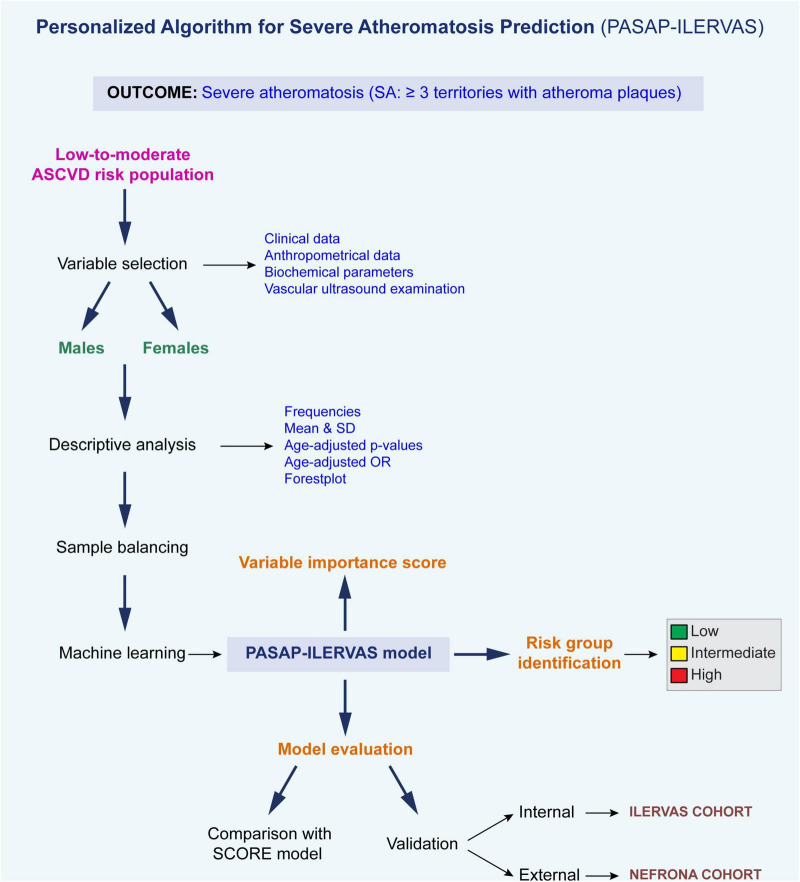
Background: Although European guidelines recommend vascular ultrasound for the assessment of cardiovascular risk in low-to-moderate risk individuals, no algorithm properly identifies patients who could benefit from it. The aim of this study is to develop a sex-specific algorithm to identify those patients, especially women who are usually underdiagnosed.
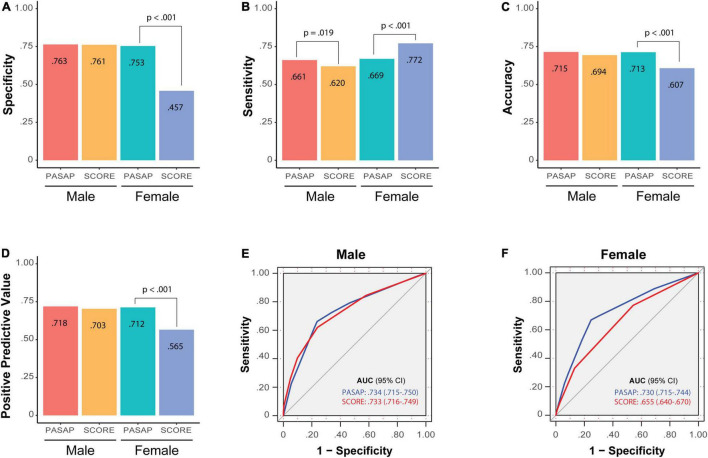
Methods: Clinical, anthropometrical, and biochemical data were combined with a 12-territory vascular ultrasound to predict severe atheromatosis (SA: ≥ 3 territories with plaque). A Personalized Algorithm for Severe Atheromatosis Prediction (PASAP-ILERVAS) was obtained by machine learning. Models were trained in the ILERVAS cohort (n = 8,330; 51% women) and validated in the control subpopulation of the NEFRONA cohort (n = 559; 47% women). Performance was compared to the Systematic COronary Risk Evaluation (SCORE) model.
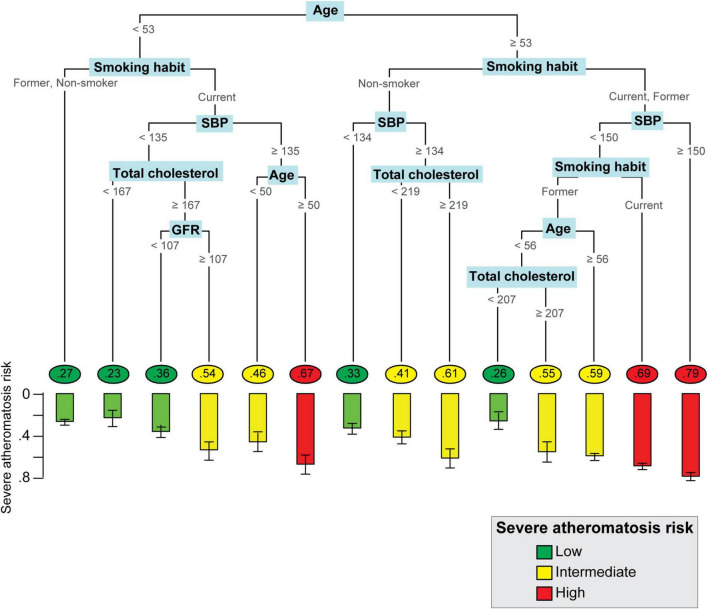
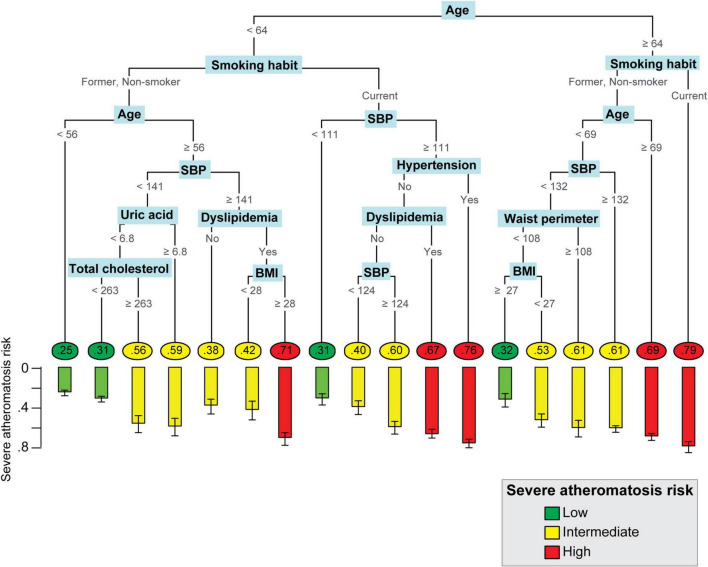
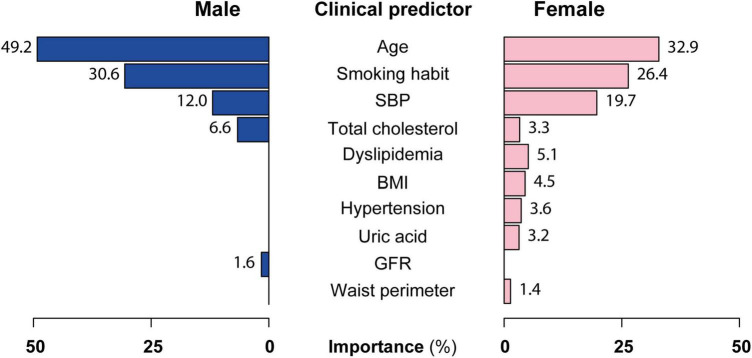
Results: The PASAP-ILERVAS is a sex-specific, easy-to-interpret predictive model that stratifies individuals according to their risk of SA in low, intermediate, or high risk. New clinical predictors beyond traditional factors were uncovered. In low- and high-risk (L&H-risk) men, the net reclassification index (NRI) was 0.044 (95% CI: 0.020-0.068), and the integrated discrimination index (IDI) was 0.038 (95% CI: 0.029-0.048) compared to the SCORE. In L&H-risk women, PASAP-ILERVAS showed a significant increase in the area under the curve (AUC, 0.074 (95% CI: 0.062-0.087), p-value: < 0.001), an NRI of 0.193 (95% CI: 0.162-0.224), and an IDI of 0.119 (95% CI: 0.109-0.129).
Conclusion: The PASAP-ILERVAS improves SA prediction, especially in women. Thus, it could reduce the number of unnecessary complementary explorations selecting patients for a further imaging study within the intermediate risk group, increasing cost-effectiveness and optimizing health resources.
Clinical trial registration: [www.ClinicalTrials.gov], identifier [NCT03228459].
Keywords: atherosclerosis; cardiovascular disease; cardiovascular risk assessment; machine learning; recursive partitioning classification trees; vascular ultrasound.
Copyright © 2022 Bermúdez-López, Martí-Antonio, Castro-Boqué, Bretones, Farràs, Torres, Pamplona, Lecube, Mauricio, Valdivielso and Fernández on behalf of the ILERVAS Project Collaborators.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Subclinical atheromatosis localization and burden in a low-to-moderate cardiovascular risk population: the ILERVAS study.Rev Esp Cardiol (Engl Ed). 2021 Dec;74(12):1042-1053. doi: 10.1016/j.rec.2020.09.015. Epub 2020 Nov 6. Rev Esp Cardiol (Engl Ed). 2021. PMID: 33162389 Clinical Trial. English, Spanish.
-
Cumulative tobacco consumption has a dose-dependent effect on atheromatosis burden and improves severe atheromatosis prediction in asymptomatic middle-aged individuals: The ILERVAS study.Atherosclerosis. 2023 Jun;375:75-83. doi: 10.1016/j.atherosclerosis.2023.05.002. Epub 2023 May 18. Atherosclerosis. 2023. PMID: 37276714
-
Characteristics of atheromatosis in the prediabetes stage: a cross-sectional investigation of the ILERVAS project.Cardiovasc Diabetol. 2019 Nov 15;18(1):154. doi: 10.1186/s12933-019-0962-6. Cardiovasc Diabetol. 2019. PMID: 31729979 Free PMC article.
-
Imaging-guided evaluation of subclinical atherosclerosis to enhance cardiovascular risk prediction in asymptomatic low-to-intermediate risk individuals: A systematic review.Prev Med. 2021 Dec;153:106819. doi: 10.1016/j.ypmed.2021.106819. Epub 2021 Sep 29. Prev Med. 2021. PMID: 34599926
-
Prognostic models for newly-diagnosed chronic lymphocytic leukaemia in adults: a systematic review and meta-analysis.Cochrane Database Syst Rev. 2020 Jul 31;7(7):CD012022. doi: 10.1002/14651858.CD012022.pub2. Cochrane Database Syst Rev. 2020. PMID: 32735048 Free PMC article.
Cited by
-
Health Equity in Clinical Research Informatics.Yearb Med Inform. 2023 Aug;32(1):138-145. doi: 10.1055/s-0043-1768720. Epub 2023 Jul 6. Yearb Med Inform. 2023. PMID: 37414033 Free PMC article. Review.
References
-
- Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. (2020) 41:111–88. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical