

Altered muscle oxidative phenotype impairs exercise tolerance but does not improve after exercise training in multiple sclerosis
- PMID: 35929063
- PMCID: PMC9530506
- DOI: 10.1002/jcsm.13050
Altered muscle oxidative phenotype impairs exercise tolerance but does not improve after exercise training in multiple sclerosis
Abstract
Background: Patients with multiple sclerosis (MS) experience reduced exercise tolerance that substantially reduces quality of life. The mechanisms underpinning exercise intolerance in MS are not fully clear. This study aimed to determine the contributions of the cardiopulmonary system and peripheral muscle in MS-induced exercise intolerance before and after exercise training.
Methods: Twenty-three patients with MS (13 women) and 20 age-matched and sex-matched healthy controls (13 women) performed a cardiopulmonary exercise test. Muscle fibre type composition, size, succinate dehydrogenase (SDH) activity, capillarity, and gene expression and proteins related to mitochondrial density were determined in vastus lateralis muscle biopsies. Nine MS patients (five women) were re-examined following a 12 week exercise training programme consisting of high-intensity cycling interval and resistance training.
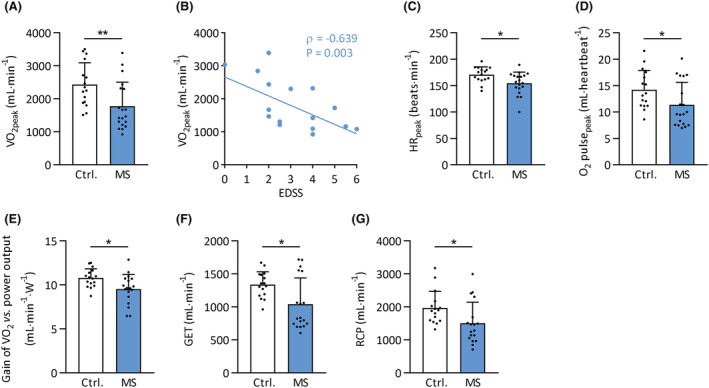
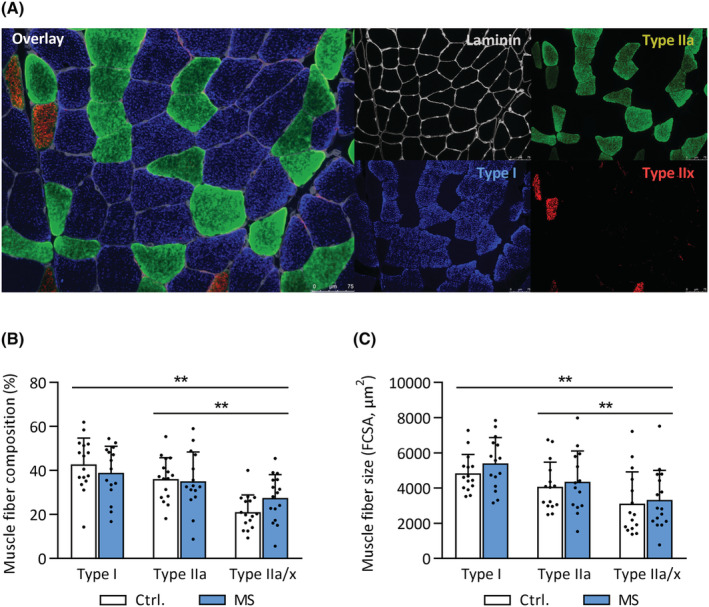
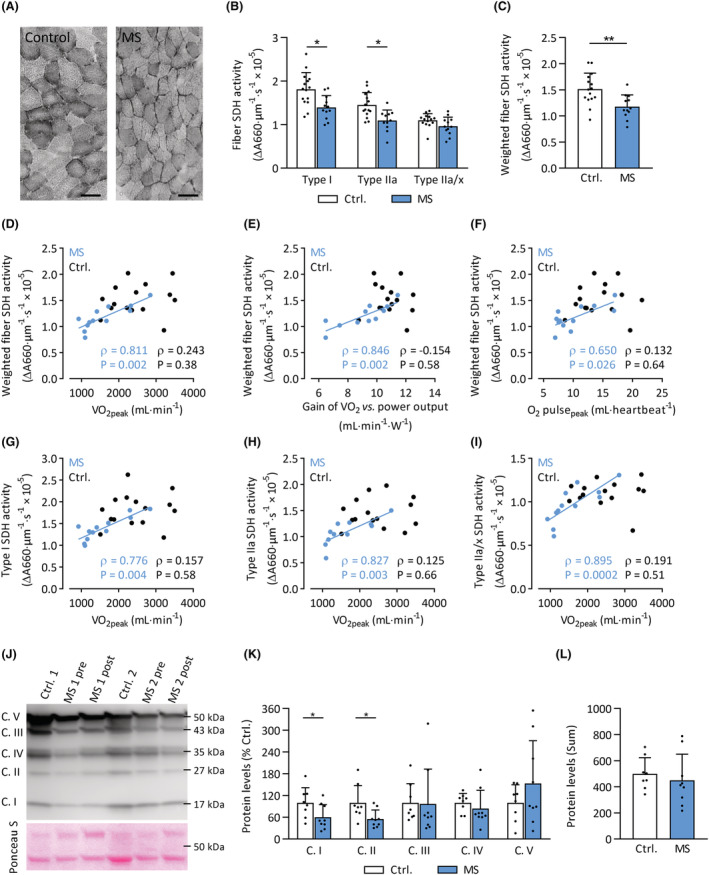
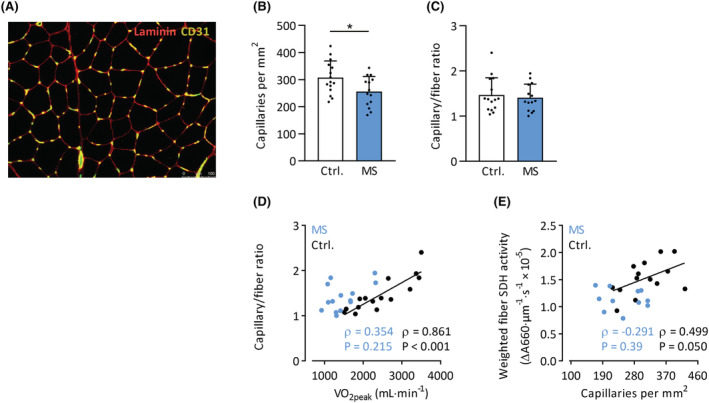
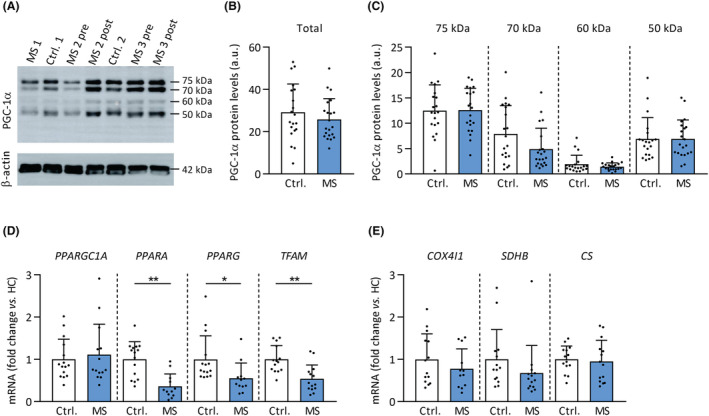
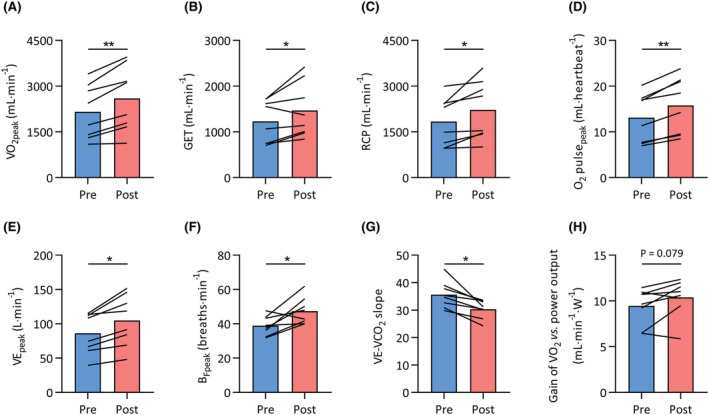
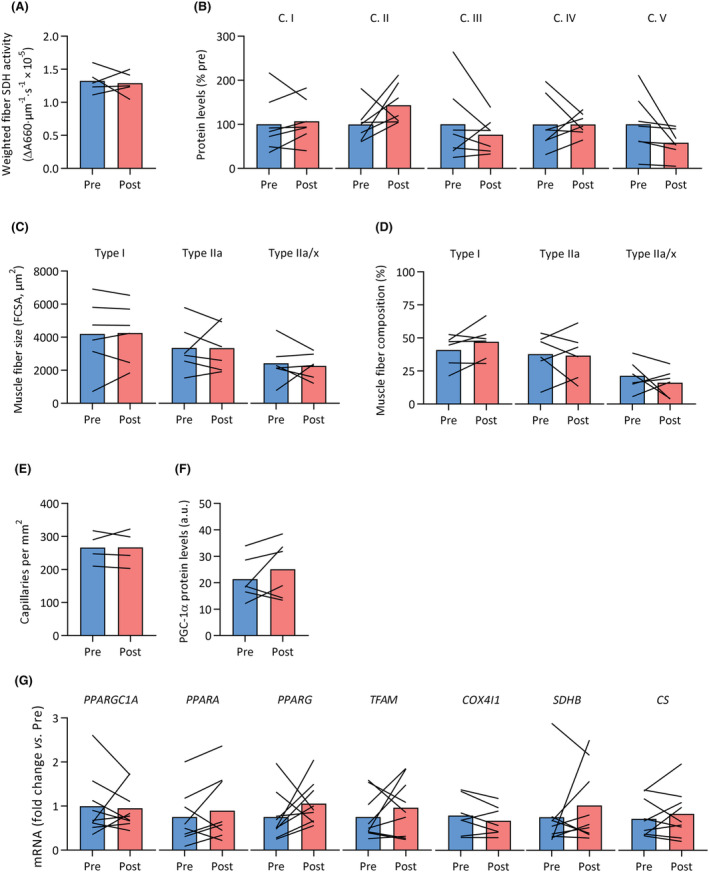
Results: Patients with MS had lower maximal oxygen uptake compared with healthy controls (V̇O2peak , 25.0 ± 8.5 vs. 35.7 ± 6.4 mL/kg/min, P < 0.001). The lower gas exchange threshold (MS: 14.5 ± 5.5 vs. controls: 19.7 ± 2.9 mL/kg/min, P = 0.01) and slope of V̇O2 versus work rate (MS: 9.5 ± 1.7 vs. controls: 10.8 ± 1.1 mL/min/W, P = 0.01) suggested an intramuscular contribution to exercise intolerance in patients with MS. Muscle SDH activity was 22% lower in MS (P = 0.004), and strongly correlated with several indices of whole-body exercise capacity in MS patients (e.g. V̇O2peak , Spearman's ρ = 0.81, P = 0.002), but not healthy controls (ρ = 0.24, P = 0.38). In addition, protein levels of mitochondrial OXPHOS complexes I (-40%, P = 0.047) and II (-45%, P = 0.026) were lower in MS patients versus controls. Muscle capillary/fibre ratio correlated with V̇O2peak in healthy controls (ρ = 0.86, P < 0.001) but not in MS (ρ = 0.35, P = 0.22), and did not differ between groups (1.41 ± 0.30 vs. 1.47 ± 0.38, P = 0.65). Expression of genes involved in mitochondrial function, such as PPARA, PPARG, and TFAM, was markedly reduced in muscle tissue samples of MS patients (all P < 0.05). No differences in muscle fibre type composition or size were observed between groups (all P > 0.05). V̇O2peak increased by 23% following exercise training in MS (P < 0.001); however, no changes in muscle capillarity, SDH activity, gene or protein expression were observed (all P > 0.05).
Conclusions: Skeletal muscle oxidative phenotype (mitochondrial complex I and II content, SDH activity) is lower in patients with MS, contributing to reduced exercise tolerance. However, skeletal muscle mitochondria appeared resistant to the beneficial effects of exercise training, suggesting that other physiological systems, at least in part, drive the improvements in exercise capacity following exercise training in MS.
Keywords: Exercise capacity; Exercise therapy; Mitochondria; Multiple sclerosis; Oxidative metabolism; Skeletal muscle.
© 2022 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by John Wiley & Sons Ltd on behalf of Society on Sarcopenia, Cachexia and Wasting Disorders.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Ontaneda D, Thompson AJ, Fox RJ, Cohen JA. Progressive multiple sclerosis: prospects for disease therapy, repair, and restoration of function. Lancet 2017;389:1357–1366. - PubMed
-
- Casey B, Coote S, Galvin R, Donnelly A. Objective physical activity levels in people with multiple sclerosis: meta‐analysis. Scand J Med Sci Sports 2018;28:1960–1969. - PubMed
-
- Marrie RA. Comorbidity in multiple sclerosis: Past, present and future. Clin Invest Med 2019;42:E5–E12. - PubMed
-
- Motl RW, Dlugonski D, Pilutti L, Sandroff B, McAuley E. Premorbid physical activity predicts disability progression in relapsing–remitting multiple sclerosis. J Neurol Sci 2012;323:123–127. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
