

COVID-19 during the index hospital admission confers a 'double-hit' effect on hip fracture patients and is associated with a two-fold increase in 1-year mortality risk
- PMID: 35929286
- PMCID: PMC9538200
- DOI: 10.1002/msc.1674
COVID-19 during the index hospital admission confers a 'double-hit' effect on hip fracture patients and is associated with a two-fold increase in 1-year mortality risk
Abstract
Purpose: The aims were to: (1) determine 1-year mortality rates for hip fracture patients during the first UK COVID-19 wave, and (2) assess mortality risk associated with COVID-19.
Methods: A nationwide multicentre cohort study was conducted of all patients presenting to 17 hospitals in March-April 2020. Follow-up data were collected one year after initial hip fracture ('index') admission, including: COVID-19 status, readmissions, mortality, and cause of death.
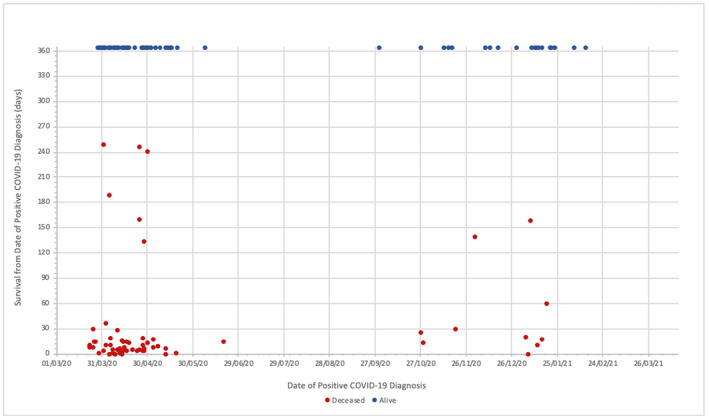
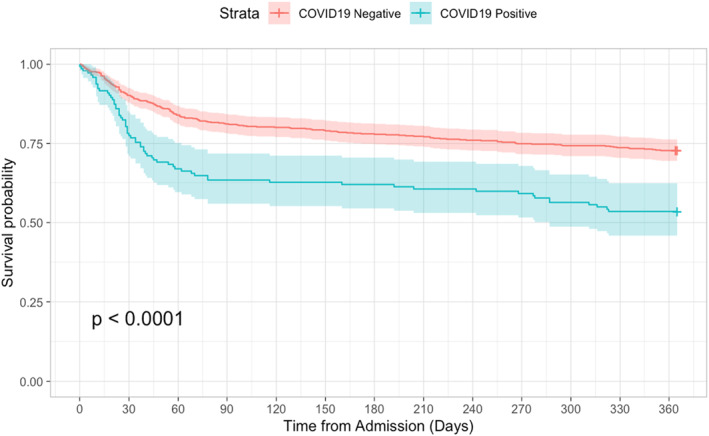
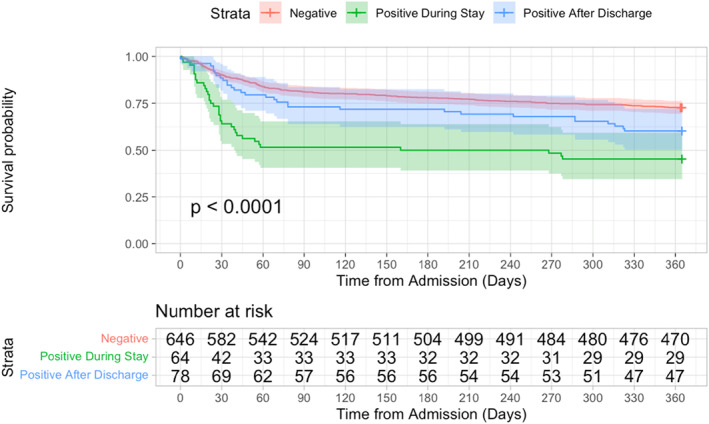
Results: Data were available for 788/833 (94.6%) patients. One-year mortality was 242/788 (30.7%), and the prevalence of COVID-19 within 365 days of admission was 142/788 (18.0%). One-year mortality was higher for patients with COVID-19 (46.5% vs. 27.2%; p < 0.001), and highest for those COVID-positive during index admission versus after discharge (54.7% vs. 39.7%; p = 0.025). Anytime COVID-19 was independently associated with 50% increased mortality risk within a year of injury (HR 1.50, p = 0.006); adjusted mortality risk doubled (HR 2.03, p < 0.001) for patients COVID-positive during index admission. No independent association was observed between mortality risk and COVID-19 diagnosed following discharge (HR 1.16, p = 0.462). Most deaths (56/66; 84.8%) in COVID-positive patients occurred within 30 days of COVID-19 diagnosis (median 11.0 days). Most cases diagnosed following discharge from the admission hospital occurred in downstream hospitals.
Conclusion: Almost half the patients that had COVID-19 within 365 days of fracture had died within one year of injury versus 27.2% of COVID-negative patients. Only COVID-19 diagnosed during the index admission was associated independently with an increased likelihood of death, indicating that infection during this time may represent a 'double-hit' insult, and most COVID-related deaths occurred within 30 days of diagnosis.
Keywords: COVID-19; audit; frailty; hip fracture; mortality; nosocomial; orthopaedics.
© 2022 The Authors. Musculoskeletal Care published by John Wiley & Sons Ltd.
Conflict of interest statement
All authors declare that they have no conflict of interest or financial/non‐financial interests related to this work.
Figures
References
-
- BGS . (2020). COVID‐19: Managing the COVID‐19 pandemic in care homes for older people. British Geriatrics Society (BGS).
-
- Caldicott, F. (1999). The Caldicott report. IHRIM, 40(2), 17–19. - PubMed
-
- Clement, N. D. , Hall, A. J. , Kader, N. , Ollivere, B. , Oussedik, S. , Kader, D. F. , Deehan, D. J. , & Duckworth, A. D. (2021). The rate of COVID‐19 and associated mortality after elective hip and knee arthroplasty prior to cessation of elective services in UK. The Bone & Joint Journal, 103‐B(4), 681–688. 10.1302/0301-620X.103B.BJJ-2020-1776.R1 - DOI - PubMed
-
- Clement, N. D. , Hall, A. J. , Makaram, N. S. , Robinson, P. G. , Patton, R. F. L. , Moran, M. , Macpherson, G. J. , Duckworth, A. D. , & Jenkins, P. J. (2020). IMPACT‐restart: The influence of COVID‐19 on postoperative mortality and risk factors associated with SARS‐CoV‐2 infection after orthopaedic and trauma surgery. The Bone & Joint Journal, 102‐B(12), 1774–1781. 10.1302/0301-620X.102B12.BJJ-2020-1395.R2 - DOI - PubMed
-
- Clement, N. D. , Ng, N. , Simpson, C. J. , Patton, R. F. L. , Hall, A. J. , Simpson, A. H. R. W. , & Duckworth, A. D. (2020). The prevalence, mortality, and associated risk factors for developing COVID‐19 in hip fracture patients: A systematic review and meta‐analysis. Bone and Joint Research, 9(12), 873–883. 10.1302/2046-3758.912.BJR-2020-0473.R1 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
