

Trends, Predictors, and Outcomes of 30-Day Readmission With Heart Failure After Transcatheter Aortic Valve Replacement: Insights From the US Nationwide Readmission Database
- PMID: 35929464
- PMCID: PMC9496292
- DOI: 10.1161/JAHA.121.024890
Trends, Predictors, and Outcomes of 30-Day Readmission With Heart Failure After Transcatheter Aortic Valve Replacement: Insights From the US Nationwide Readmission Database
Abstract
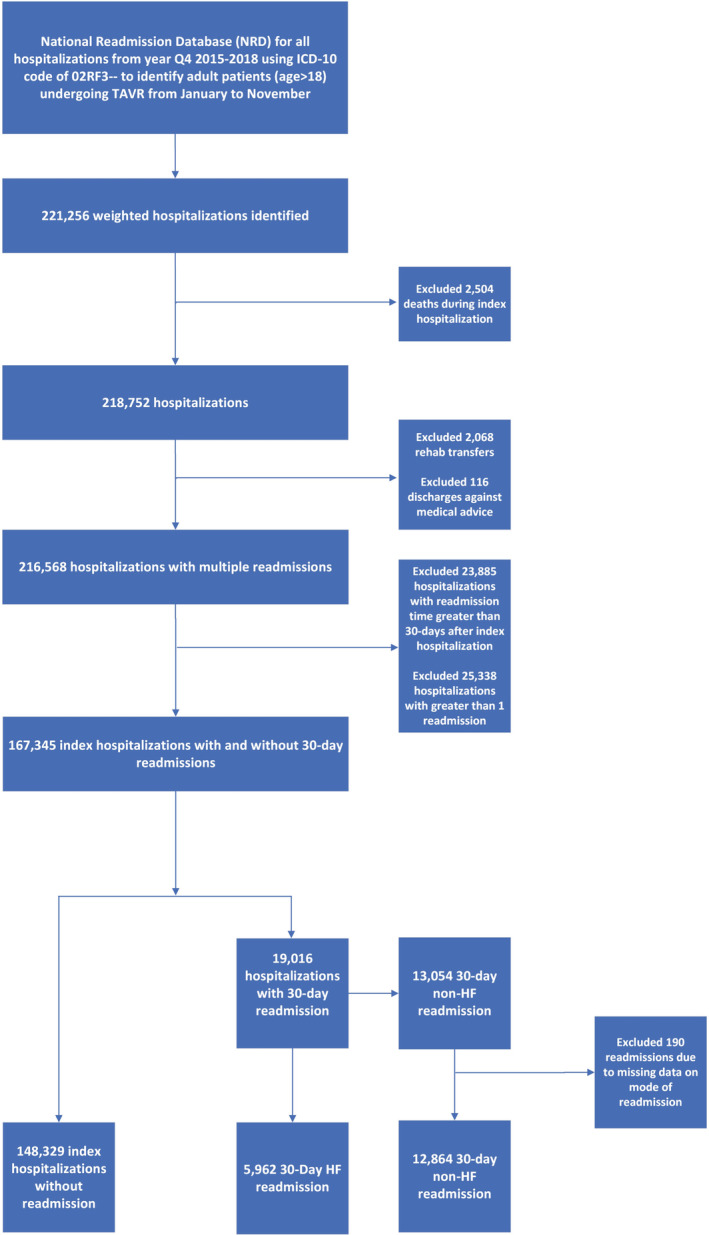
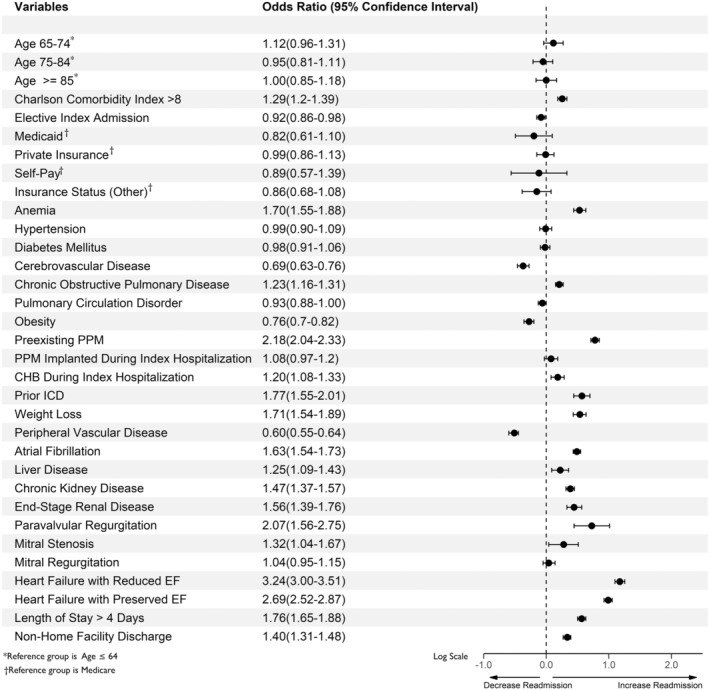
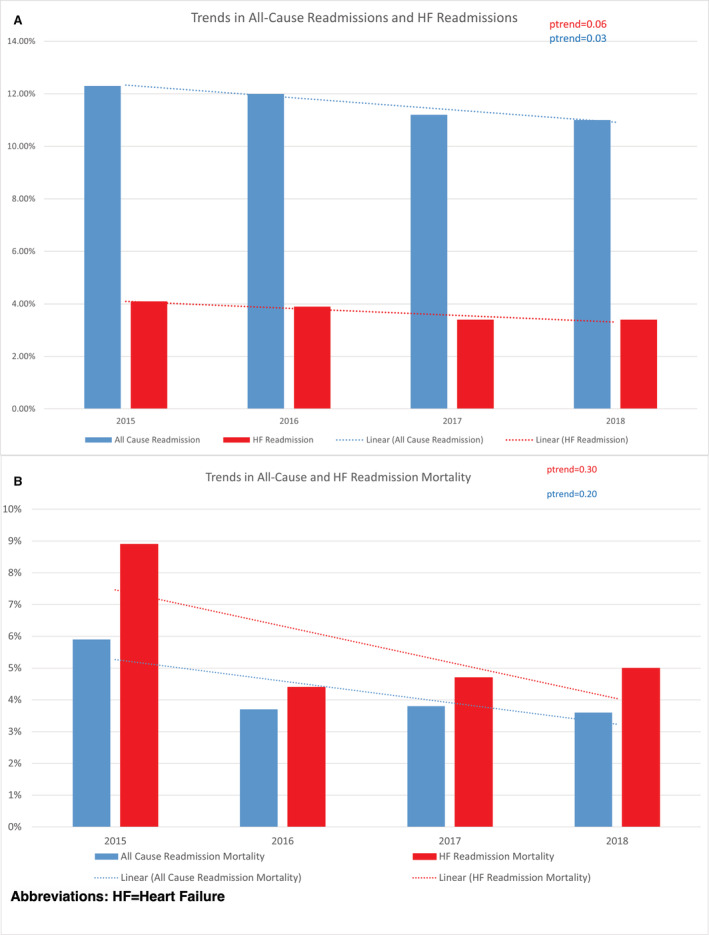
BACKGROUND Data on trends, predictors, and outcomes of heart failure (HF) readmissions after transcatheter aortic valve replacement (TAVR) remain limited. Moreover, the relationship between hospital TAVR discharge volume and HF readmission outcomes has not been established. METHODS AND RESULTS The Nationwide Readmission Database was used to identify 30-day readmissions for HF after TAVR from October 1, 2015, to November 30, 2018, using International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) codes. A total of 167 345 weighted discharges following TAVR were identified. The all-cause readmission rate within 30 days of discharge was 11.4% (19 016). Of all the causes of 30-day rehospitalizations, HF comprised 31.4% (5962) of all causes. The 30-day readmission rate for HF did not show a significant decline during the study period (Ptrend=0.06); however, all-cause readmission rates decreased significantly (Ptrend=0.03). HF readmissions were comparable between high- and low-volume TAVR centers. Charlson Comorbidity Index >8, length of stay >4 days during the index hospitalization, chronic obstructive pulmonary disease, atrial fibrillation, chronic HF, preexisting pacemaker, complete heart block during index hospitalization, paravalvular regurgitation, chronic kidney disease, and end-stage renal disease were independent predictors of 30-day HF readmission after TAVR. HF readmissions were associated with higher mortality rates when compared with non-HF readmissions (4.9% versus 3.3%; P<0.01). Each HF readmission within 30 days was associated with an average increased cost of $13 000 more than for each non-HF readmission. CONCLUSIONS During the study period from 2015 to 2018, 30-day HF readmissions after TAVR remained steady despite all-cause readmissions decreasing significantly. All-cause readmission mortality and HF readmission mortality also showed a nonsignificant downtrend. HF readmissions were comparable across low-, medium-, and high-volume TAVR centers. HF readmission was associated with increased mortality and resource use attributed to the increased costs of care compared with non-HF readmission. Further studies are needed to identify strategies to decrease the burden of HF readmissions and related mortality after TAVR.
Keywords: TAVI; TAVR; heart failure; transcatheter aortic valve implantation; transcatheter aortic valve replacement.
Figures
References
-
- Sanchez CE, Hermiller JBJ, Pinto DS, Chetcuti SJ, Arshi A, Forrest JK, Huang J, Yakubov SJ. Predictors and risk calculator of early unplanned hospital readmission following contemporary self‐expanding transcatheter aortic valve replacement from the STS/ACC TVT registry. Cardiovasc Revasc Med. 2020;21:263–270. doi: 10.1016/j.carrev.2019.05.032 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
