

Postoperative Packing of Perianal Abscess Cavities (PPAC2): randomized clinical trial
- PMID: 35929816
- PMCID: PMC10364677
- DOI: 10.1093/bjs/znac225
Postoperative Packing of Perianal Abscess Cavities (PPAC2): randomized clinical trial
Abstract
Background: Perianal abscess is common. Traditionally, postoperative perianal abscess cavities are managed with internal wound packing, a practice not supported by evidence. The aim of this randomized clinical trial (RCT) was to assess if non-packing is less painful and if it is associated with adverse outcomes.
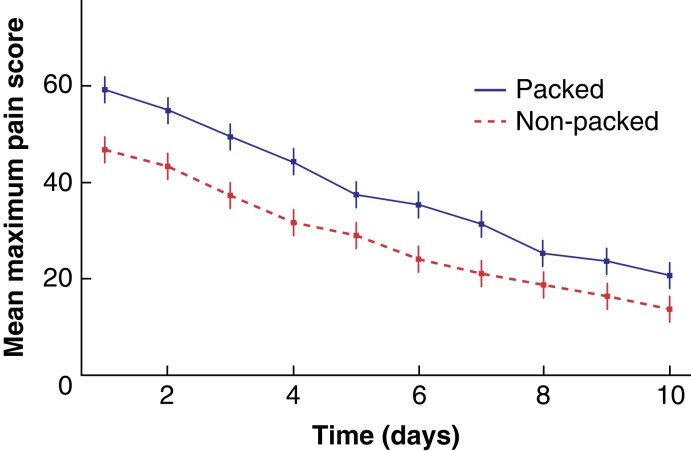
Methods: The Postoperative Packing of Perianal Abscess Cavities (PPAC2) trial was a multicentre, RCT (two-group parallel design) of adult participants admitted to an NHS hospital for incision and drainage of a primary perianal abscess. Participants were randomized 1:1 (via an online system) to receive continued postoperative wound packing or non-packing. Blinded data were collected via symptom diaries, telephone, and clinics over 6 months. The objective was to determine whether non-packing of perianal abscess cavities is less painful than packing, without an increase in perianal fistula or abscess recurrence. The primary outcome was pain (mean maximum pain score on a 100-point visual analogue scale).
Results: Between February 2018 and March 2020, 433 participants (mean age 42 years) were randomized across 50 sites. Two hundred and thirteen participants allocated to packing reported higher pain scores than 220 allocated to non-packing (38.2 versus 28.2, mean difference 9.9; P < 0.0001). The occurrence of fistula-in-ano was low in both groups: 32/213 (15 per cent) in the packing group and 24/220 (11 per cent) in the non-packing group (OR 0.69, 95 per cent c.i. 0.39 to 1.22; P = 0.20). The proportion of patients with abscess recurrence was also low: 13/223 (6 per cent) in the non-packing group and 7/213 (3 per cent) in the packing group (OR 1.85, 95 per cent c.i. 0.72 to 4.73; P = 0.20).
Conclusion: Avoiding abscess cavity packing is less painful without a negative morbidity risk.
Registration number: ISRCTN93273484 (https://www.isrctn.com/ISRCTN93273484).
Registration number: NCT03315169 (http://clinicaltrials.gov).
Plain language summary
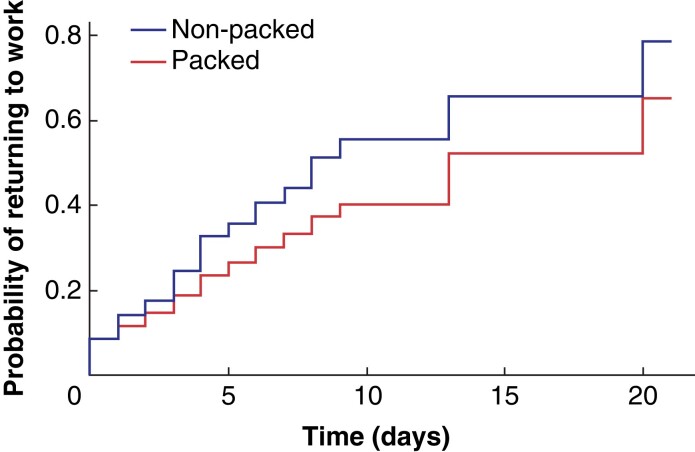
Perianal abscess is a common, painful condition due to infection and swelling around the anus caused by blockage of the anal glands. The treatment of perianal abscess has stayed the same for over 50 years. An operation is performed under general anaesthetic to cut the skin and drain the infection. This is followed by continued internal dressing (packing) of the remaining cavity (hole) until the skin has healed over. Packing changes are needed multiple times a week for several weeks. Packing is the accepted treatment as it is believed to reduce the chance of the abscess coming back, and also reduces the chance of perianal fistula forming. There are no medical studies to support this idea. Perianal fistula (an abnormal passage between the skin around the anus, and the inside of the anal canal or rectum) is a long-term condition, which causes pain, and pus (and sometimes faeces) discharge, and often needs another operation (or multiple operations) to fix it. This trial was performed to demonstrate if no packing of a perianal abscess would result in a reduction of pain, with no increase in unwanted abscess recurrences and fistulas, in comparison to the standard treatment of packing. The trial recruited 433 people, who were randomly chosen to enter one of two groups; one to have their wound packed and the other to have no packing of the wound. After being discharged from hospital following surgery, the patients attended or were visited by a community nurse for the dressing to be changed or wound packed. Each patient provided information on pain from their wound, including worst pain each day and pain before, during, and after the changing of their dressing or packing. This and other information was gathered for the first 10 days after surgery and periodically until 6 months after surgery. The no-packing group experienced much less pain than the packing group. There was no difference in abscess recurrence and fistula formation between the non-packing and packing groups. The findings demonstrate that no packing of perianal abscess wounds after drainage operation is the best treatment.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures

References
-
- Sahnan K, Askari A, Adegbola SO, Tozer PJ, Phillips RKS, Hart A et al. Natural history of anorectal sepsis. Br J Surg 2017;104:1857–1865 - PubMed
-
- Eisenhammer S. The final evaluation and classification of the surgical treatment of the primary anorectal cryptoglandular intermuscular (intersphincteric) fistulous abscess and fistula. Dis Colon Rectum 1978;21:237–254 - PubMed
-
- Hamadani A, Haigh PI, Liu ILA, Abbas MA. Who is at risk for developing chronic anal fistula or recurrent anal sepsis after initial perianal abscess? Dis Colon Rectum 2009;52:217–221 - PubMed
-
- Parks AG, Gordon PH, Hardcastle JD. A classification of fistula-in-ano. Br J Surg 1976;63:1–12 - PubMed
-
- Sainio P. Fistula-in-ano in a defined population. Incidence and epidemiological aspects. Ann Chir Gynaecol 1984;73:219–224 - PubMed
