

Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU: comparison of machine learning methods and conventional regression
- PMID: 35930309
- PMCID: PMC9359199
- DOI: 10.1080/0886022X.2022.2107542
Predicting renal function recovery and short-term reversibility among acute kidney injury patients in the ICU: comparison of machine learning methods and conventional regression
Abstract
Background: Acute kidney injury (AKI) is one of the most frequent complications of critical illness. We aimed to explore the predictors of renal function recovery and the short-term reversibility after AKI by comparing logistic regression with four machine learning models.
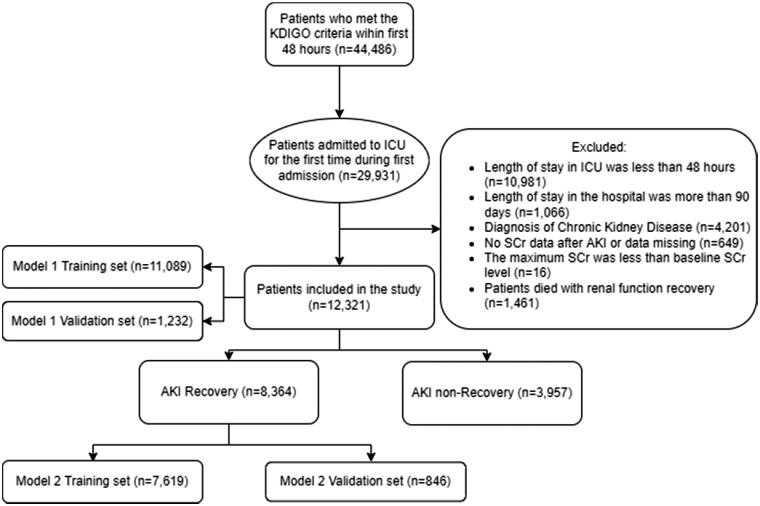
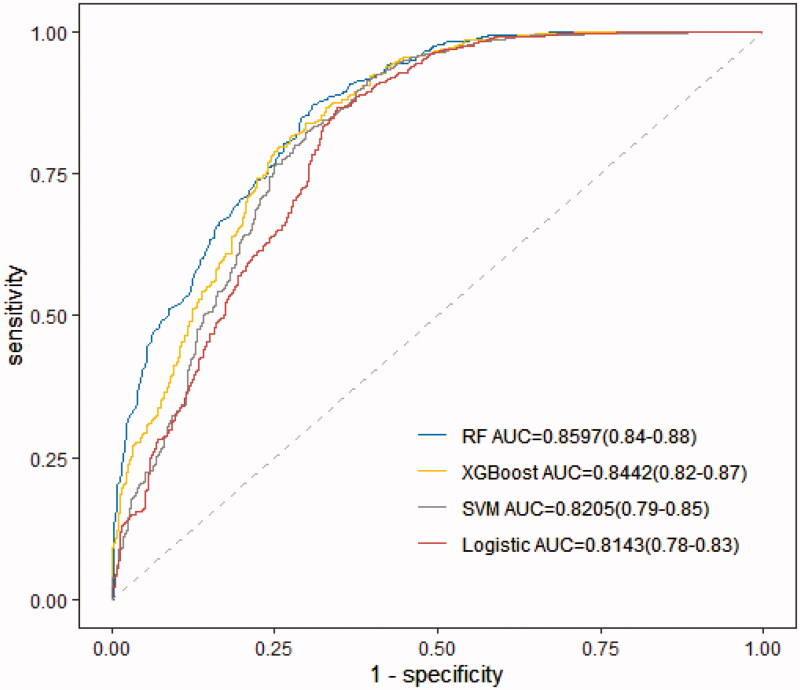
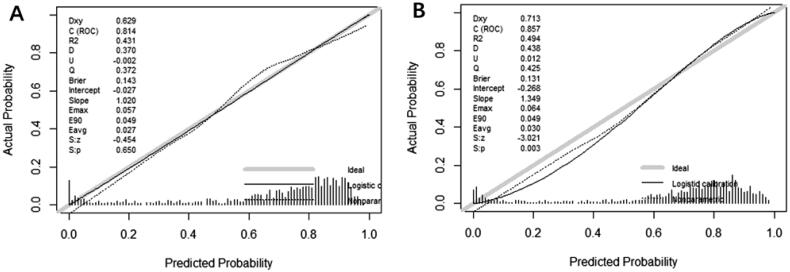
Methods: We reviewed patients who were diagnosed with AKI in the MIMIC-IV database between 2008 and 2019. Recovery from AKI within 72 h of the initiating event was typically recognized as the short-term reversal of AKI. Conventional logistic regression and four different machine algorithms (XGBoost algorithm model, Bayesian networks [BNs], random forest [RF] model, and support vector machine [SVM] model) were used to develop and validate prediction models. The performance measures were compared through the area under the receiver operating characteristic curve (AU-ROC), calibration curves, and 10-fold cross-validation.
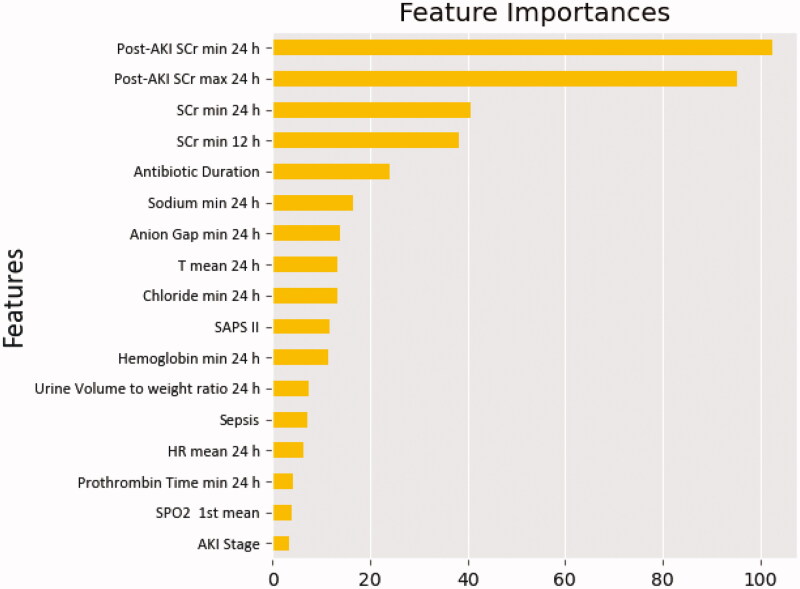
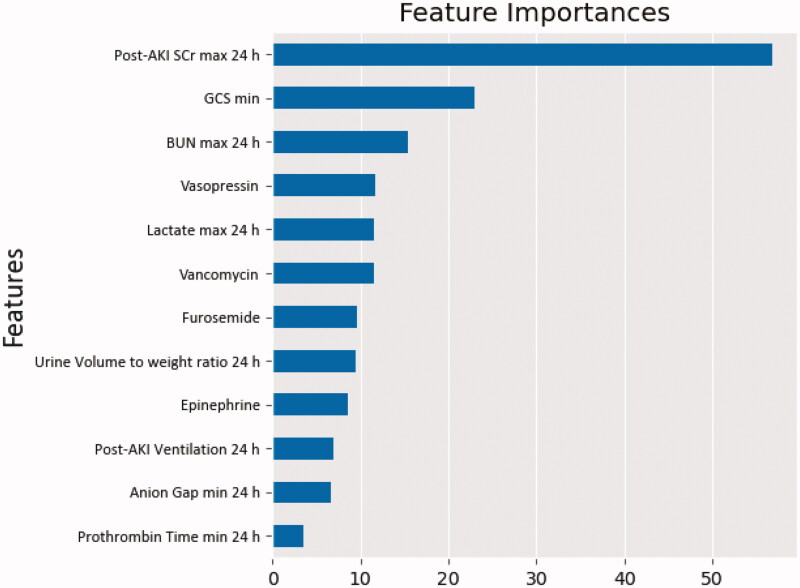
Results: A total of 12,321 critically ill adult AKI patients were included in our analysis cohort. The renal function recovery rate after AKI was 67.9%. The maximum and minimum serum creatinine (SCr) within 24 h of AKI diagnosis, the minimum SCr within 24 and 12 h, and antibiotics usage duration were independently associated with renal function recovery after AKI. Among the 8364 recovered patients, the maximum SCr within 24 h of AKI diagnosis, the minimum Glasgow Coma Scale (GCS) score, the maximum blood urea nitrogen (BUN) within 24 h, vasopressin and vancomycin usage, and the maximum lactate within 24 h were the top six predictors for short-term reversibility of AKI. The RF model presented the best performance for predicting both renal functional recovery (AU-ROC [0.8295 ± 0.01]) and early recovery (AU-ROC [0.7683 ± 0.03]) compared with the conventional logistic regression model.
Conclusions: The maximum SCr within 24 h of AKI diagnosis was a common independent predictor of renal function recovery and the short-term reversibility of AKI. The RF machine learning algorithms showed a superior ability to predict the prognosis of AKI patients in the ICU compared with the traditional regression models. These models may prove to be clinically helpful and can assist clinicians in providing timely interventions, potentially leading to improved prognoses.
Keywords: Acute kidney injury; machine learning; renal function recovery; renal function recovery time.
Conflict of interest statement
No potential conflict of interest was reported by the author(s).
Figures
References
-
- Hoste EAJ, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–1423. - PubMed
-
- Chertow GM, Levy EM, Hammermeister KE, et al. Independent association between acute renal failure and mortality following cardiac surgery. Am J Med. 1998;104(4):343–348. - PubMed
-
- Chertow GM, Burdick E, Honour M, et al. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365–3370. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources