

A change of heart: Mechanisms of cardiac adaptation to acute and chronic hypoxia
- PMID: 35930370
- PMCID: PMC9544656
- DOI: 10.1113/JP281724
A change of heart: Mechanisms of cardiac adaptation to acute and chronic hypoxia
Abstract
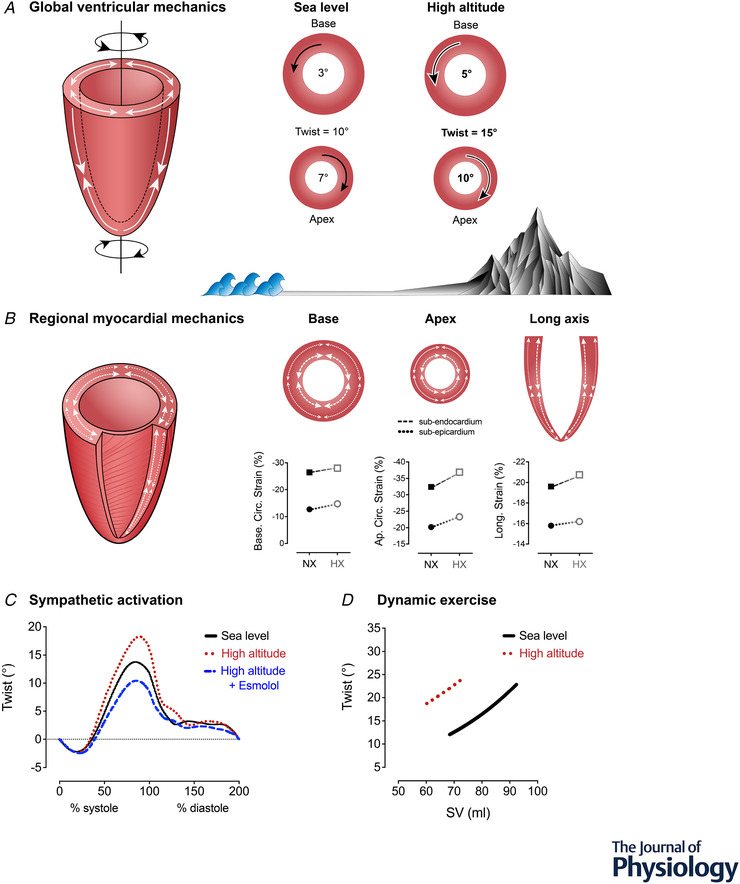
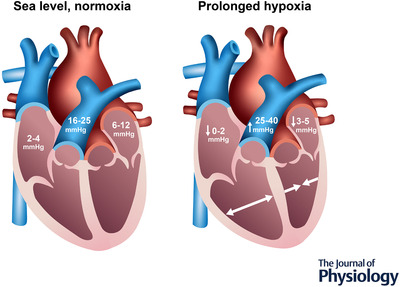
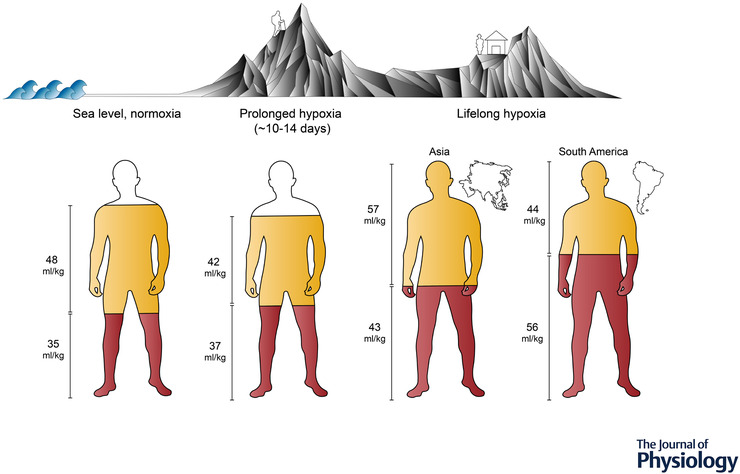
Over the last 100 years, high-altitude researchers have amassed a comprehensive understanding of the global cardiac responses to acute, prolonged and lifelong hypoxia. When lowlanders are exposed to hypoxia, the drop in arterial oxygen content demands an increase in cardiac output, which is facilitated by an elevated heart rate at the same time as ventricular volumes are maintained. As exposure is prolonged, haemoconcentration restores arterial oxygen content, whereas left ventricular filling and stroke volume are lowered as a result of a combination of reduced blood volume and hypoxic pulmonary vasoconstriction. Populations native to high-altitude, such as the Sherpa in Asia, exhibit unique lifelong or generational adaptations to hypoxia. For example, they have smaller left ventricular volumes compared to lowlanders despite having larger total blood volume. More recent investigations have begun to explore the mechanisms underlying such adaptive responses by combining novel imaging techniques with interventions that manipulate cardiac preload, afterload, and/or contractility. This work has revealed the contributions and interactions of (i) plasma volume constriction; (ii) sympathoexcitation; and (iii) hypoxic pulmonary vasoconstriction with respect to altering cardiac loading, or otherwise preserving or enhancing biventricular systolic and diastolic function even amongst high altitude natives with excessive erythrocytosis. Despite these advances, various areas of investigation remain understudied, including potential sex-related differences in response to high altitude. Collectively, the available evidence supports the conclusion that the human heart successfully adapts to hypoxia over the short- and long-term, without signs of myocardial dysfunction in healthy humans, except in very rare cases of maladaptation.
Keywords: adaptation; altitude; blood volume; cardiac function; hypoxaemia; hypoxia; pulmonary hypoxic vasoconstriction; twist.
© 2022 The Authors. The Journal of Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Figures
Similar articles
-
Short-term adaptation and chronic cardiac remodelling to high altitude in lowlander natives and Himalayan Sherpa.Exp Physiol. 2015 Nov;100(11):1242-6. doi: 10.1113/expphysiol.2014.082503. Epub 2014 Nov 20. Exp Physiol. 2015. PMID: 26575341 Review.
-
Ventricular structure, function, and mechanics at high altitude: chronic remodeling in Sherpa vs. short-term lowlander adaptation.J Appl Physiol (1985). 2014 Aug 1;117(3):334-43. doi: 10.1152/japplphysiol.00233.2014. Epub 2014 May 29. J Appl Physiol (1985). 2014. PMID: 24876358 Free PMC article.
-
Influence of iron manipulation on hypoxic pulmonary vasoconstriction and pulmonary reactivity during ascent and acclimatization to 5050 m.J Physiol. 2021 Mar;599(5):1685-1708. doi: 10.1113/JP281114. Epub 2021 Feb 3. J Physiol. 2021. PMID: 33442904
-
The influence of hemoconcentration on hypoxic pulmonary vasoconstriction in acute, prolonged, and lifelong hypoxemia.Am J Physiol Heart Circ Physiol. 2021 Oct 1;321(4):H738-H747. doi: 10.1152/ajpheart.00357.2021. Epub 2021 Aug 27. Am J Physiol Heart Circ Physiol. 2021. PMID: 34448634
-
Control of breathing and the circulation in high-altitude mammals and birds.Comp Biochem Physiol A Mol Integr Physiol. 2015 Aug;186:66-74. doi: 10.1016/j.cbpa.2014.10.009. Epub 2014 Oct 23. Comp Biochem Physiol A Mol Integr Physiol. 2015. PMID: 25446936 Review.
Cited by
-
Impact of homeostatic body hydration status, evaluated by hemodynamic measures, on different pain sensitization paths to a chronic pain syndrome.Sci Rep. 2024 Jan 22;14(1):1908. doi: 10.1038/s41598-024-52419-3. Sci Rep. 2024. PMID: 38253727 Free PMC article.
-
Sex-related Differences in Loop Gain during High-Altitude Sleep-disordered Breathing.Ann Am Thorac Soc. 2023 Aug;20(8):1192-1200. doi: 10.1513/AnnalsATS.202211-918OC. Ann Am Thorac Soc. 2023. PMID: 37000675 Free PMC article.
-
Geographic Variation in Epigenetic Responses to Hypoxia in Deer Mice (Peromyscus maniculatus) Distributed Along an Elevational Gradient.Mol Ecol. 2025 May;34(9):e17752. doi: 10.1111/mec.17752. Epub 2025 Mar 28. Mol Ecol. 2025. PMID: 40156223 Free PMC article.
-
Long-term exposure to high-altitude hypoxic environments reduces blood pressure by inhibiting the renin-angiotensin system in rats.Front Physiol. 2025 Apr 15;16:1565147. doi: 10.3389/fphys.2025.1565147. eCollection 2025. Front Physiol. 2025. PMID: 40303590 Free PMC article.
-
Phenotypic Clustering of Beta-Thalassemia Intermedia Patients Using Cardiovascular Magnetic Resonance.J Clin Med. 2023 Oct 24;12(21):6706. doi: 10.3390/jcm12216706. J Clin Med. 2023. PMID: 37959172 Free PMC article.
References
-
- Alexander, J. K. , Hartley, L. H. , Modelski, M. , & Grover, R. F. (1967). Reduction of stroke volume during exercise in man following ascent to 3,100 m altitude. Journal of Applied Physiology, 23(6), 849–858. - PubMed
-
- Anand, I. S. , Chandrashekhar, Y. , Bali, H. K. , Wahi, P. L. , Jindal, S. K. , Malhotra, R. M. , Chauhan, S. S. , & Bhandari, R. K. (1990). Adult subacute mountain sickness—a syndrome of congestive heart failure in man at very high altitude. Lancet, 335(8689), 561–565. - PubMed
-
- Baggish, A. L. , Wolfel, E. E. , & Levine, B. D. (2013). High Altitude, Human Adaptation to Hypoxia. 103–139.
-
- Beall, C. M. (2007). Detecting natural selection in high‐altitude human populations. Respiratory Physiology & Neurobiology, 158, 161–171. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials