

Advanced cardiac imaging in the spectrum of COVID-19 related cardiovascular involvement
- PMID: 35930942
- PMCID: PMC9335398
- DOI: 10.1016/j.clinimag.2022.07.009
Advanced cardiac imaging in the spectrum of COVID-19 related cardiovascular involvement
Abstract
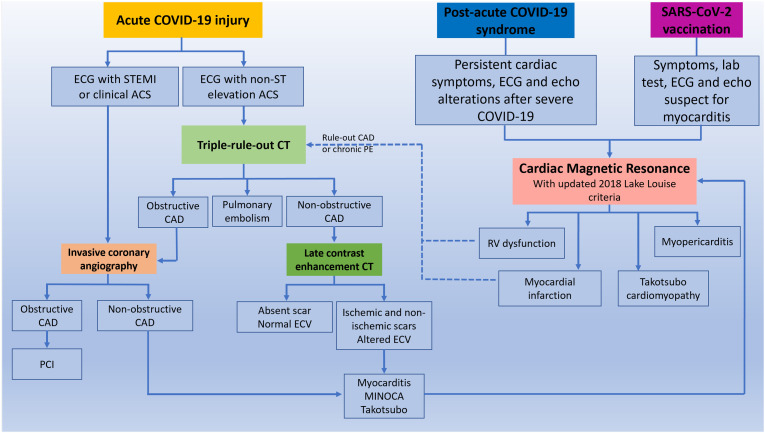
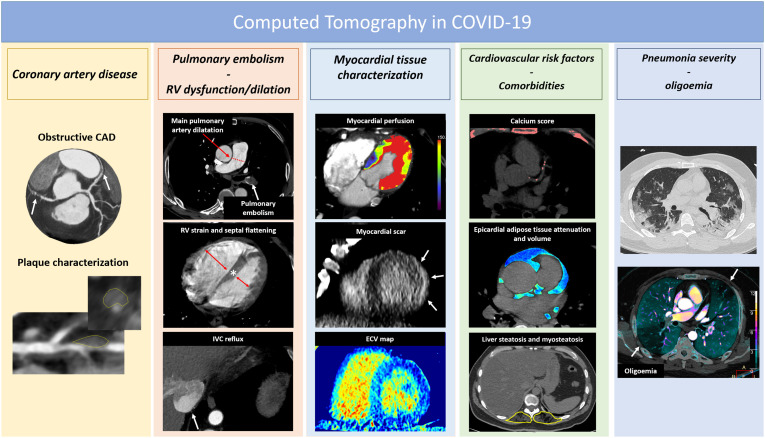
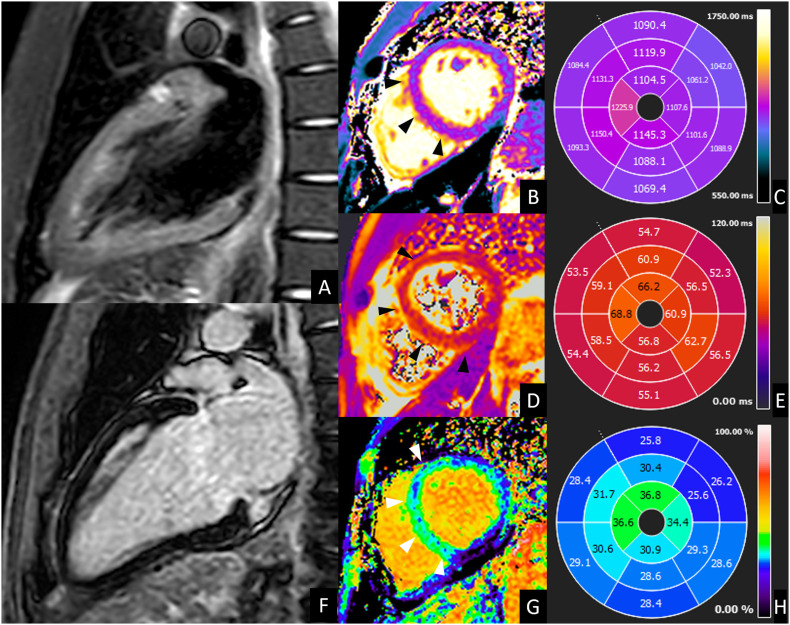
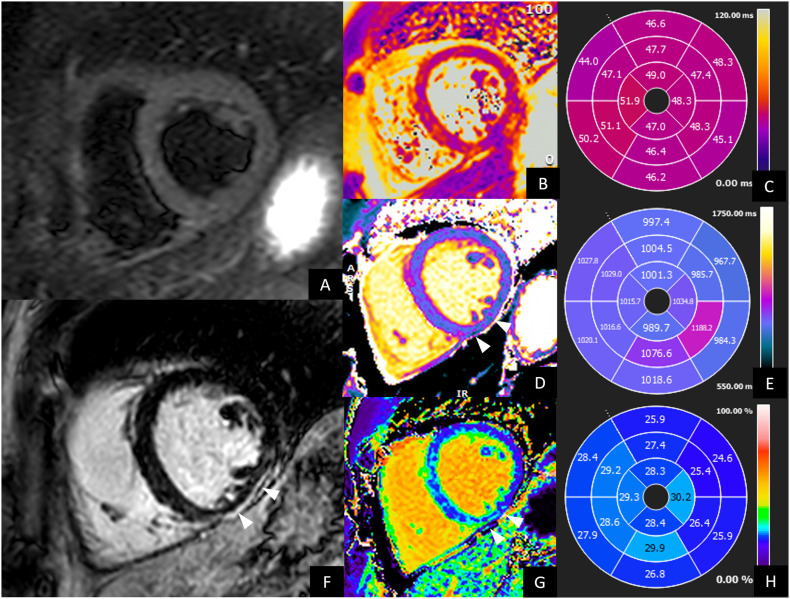
Cardiovascular involvement is a common complication of COVID-19 infection and is associated to increased risk of unfavorable outcome. Advanced imaging modalities (coronary CT angiography and Cardiac Magnetic Resonance) play a crucial role in the diagnosis, follow-up and risk stratification of patients affected by COVID-19 pneumonia with suspected cardiovascular involvement. In the present manuscript we firstly review current knowledge on the mechanisms by which SARS-CoV-2 can trigger endothelial and myocardial damage. Secondly, the implications of the cardiovascular damage on patient's prognosis are presented. Finally, we provide an overview of the main findings at advanced cardiac imaging characterizing COVID-19 in the acute setting, in the post-acute syndrome, and after vaccination, emphasizing the potentiality of CT and CMR, the indication and their clinical implications.
Keywords: COVID-19; Cardiac Magnetic Resonance; Coronary CT angiography; Myocarditis; Pulmonary embolism; Vaccine.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
