

Treatment options of metastatic and nonmetastatic VIPoma: a review
- PMID: 35931878
- PMCID: PMC9640398
- DOI: 10.1007/s00423-022-02620-7
Treatment options of metastatic and nonmetastatic VIPoma: a review
Abstract
Purpose: VIPoma belongs to the group of neuroendocrine neoplasms. These tumours are located mostly in the pancreas and produce high levels of vasoactive intestinal peptide (VIP). In most cases, a metastatic state has already been reached at the initial diagnosis, with high levels of VIP leading to a wide spectrum of presenting symptoms. These symptoms include intense diarrhoea and subsequent hypopotassaemia but also cardiac complications, with life-threatening consequences. Treatment options include symptomatic therapy, systemic chemotherapy and targeted therapy, as well as radiation and surgery. Due to the low incidence of VIPoma, there are no prospective studies or evidence-based therapeutic standards to date.
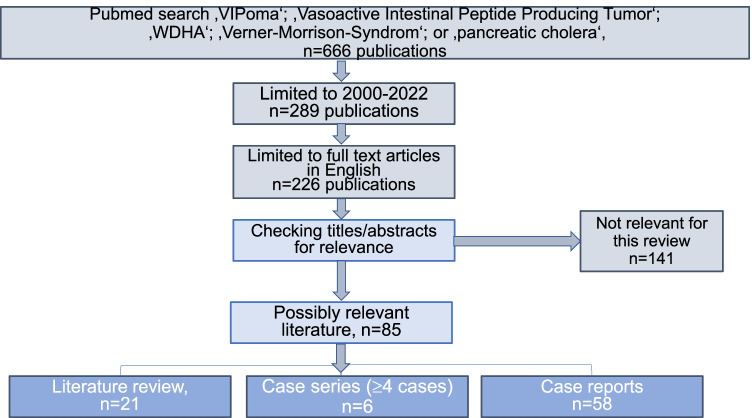
Methods: To evaluate the possible impact of different therapy strategies, we performed literature research using PubMed.
Results: All possible treatment modalities for VIPoma have at least one of two therapy goals: antisecretory effects (symptom control) and antitumoural effects (tumour burden reduction). Symptomatic therapy is the most important in the emergency setting to rehydrate, balance electrolytes and stabilise the patient. Symptomatic therapy is also of great importance perioperatively. Somatostatin analogues play a major role in symptom control, although their efficiency is often limited. Chemotherapy may be effective in reaching stable disease for a certain time period, although its impact on symptom control is limited and often delayed. Among targeted therapy options, the usage of sunitinib appears to be the most effective in terms of symptom control and showing antitumoural effects at the same time. Experience with radiation is still limited; however, local ablative procedures seem to be promising options. Peptide receptor radiotherapy (PRRT) with radiolabelled somatostatin analogues (SSAs, 177Lu-DOTATATE) offers a targeted approach, especially in patients with high somatostatin receptor density. Surgery is the first-line therapy for nonmetastatic VIPoma. Additionally, if the resection of all visible tumour lesions is possible, the surgical approach seems preferable to other strategies in highly symptomatic patients. The role of surgery in very advanced stages where only tumour debulking is possible remains debatable. However, a high rate of immediate symptom control can be achieved by tumour debulking followed by somatostatin therapy, although the impact on survival remains unclear.
Conclusion: Surgery is the only curative option for nonmetastatic VIPoma. Additionally, surgery should be a first-line therapy option for highly symptomatic patients, especially if the resection of all tumour lesions (primary tumour and metastasis) is achievable. In frail patients, other modalities can be used.
Keywords: Metastasis; Treatment; VIP; VIPoma.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Gardner JD, Cerda JJ. In vitro inhibition of intestinal fluid and electrolyte transfer by a non-beta islet cell tumor. Proc Soc Exp Biol Med. 1966;123(2):361–364. - PubMed
-
- Hahm SH, Eiden LE. Cis-regulatory elements controlling basal and inducible VIP gene transcription. Ann N Y Acad Sci. 1998;865:10–26. - PubMed
-
- Henning RJ, Sawmiller DR. Vasoactive intestinal peptide: cardiovascular effects. Cardiovasc Res. 2001;49(1):27–37. - PubMed
-
- Verner JV, Morrison AB. Islet cell tumor and a syndrome of refractory watery diarrhea and hypokalemia. Am J Med. 1958;25(3):374–380. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
