

Protocol and programme factors associated with referral and loss to follow-up from newborn hearing screening: a systematic review
- PMID: 35932008
- PMCID: PMC9354382
- DOI: 10.1186/s12887-022-03218-0
Protocol and programme factors associated with referral and loss to follow-up from newborn hearing screening: a systematic review
Abstract
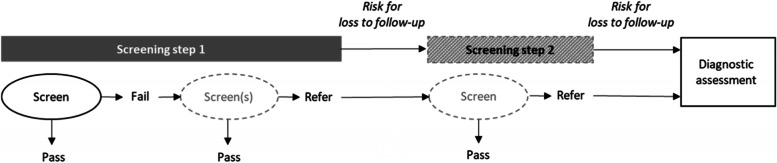
Background: An effective newborn hearing screening programme has low referral rate and low loss to follow-up (LTFU) rate after referral from initial screening. This systematic review identified studies evaluating the effect of protocol and programme factors on these two outcomes, including the screening method used and the infant group.
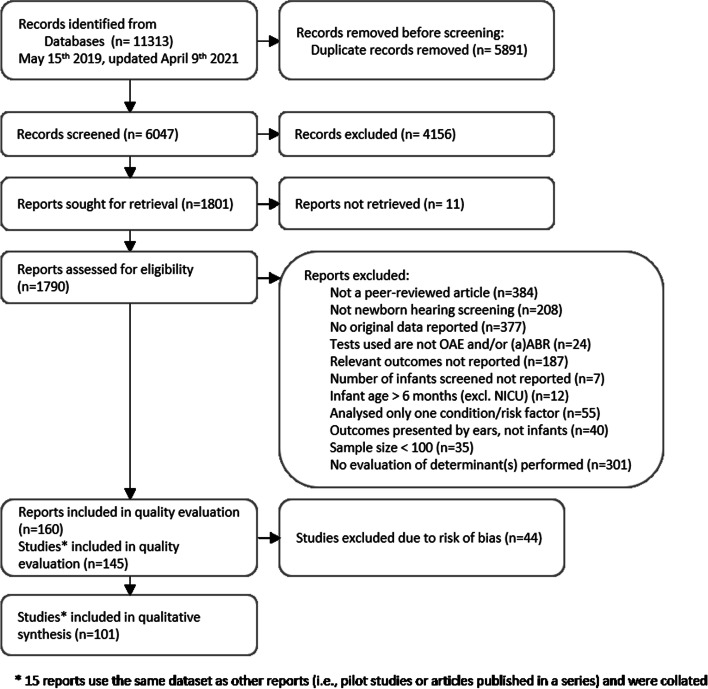
Methods: Five databases were searched (latest: April 2021). Included studies reported original data from newborn hearing screening and described the target outcomes against a protocol or programme level factor. Studies were excluded if results were only available for one risk condition, for each ear, or for < 100 infants, or if methodological bias was observed. Included studies were evaluated for quality across three domains: sample, screening and outcome, using modified criteria from the Ottawa-Newcastle and QUADAS-2 scales. Findings from the included studies were synthesised in tables, figures and text.
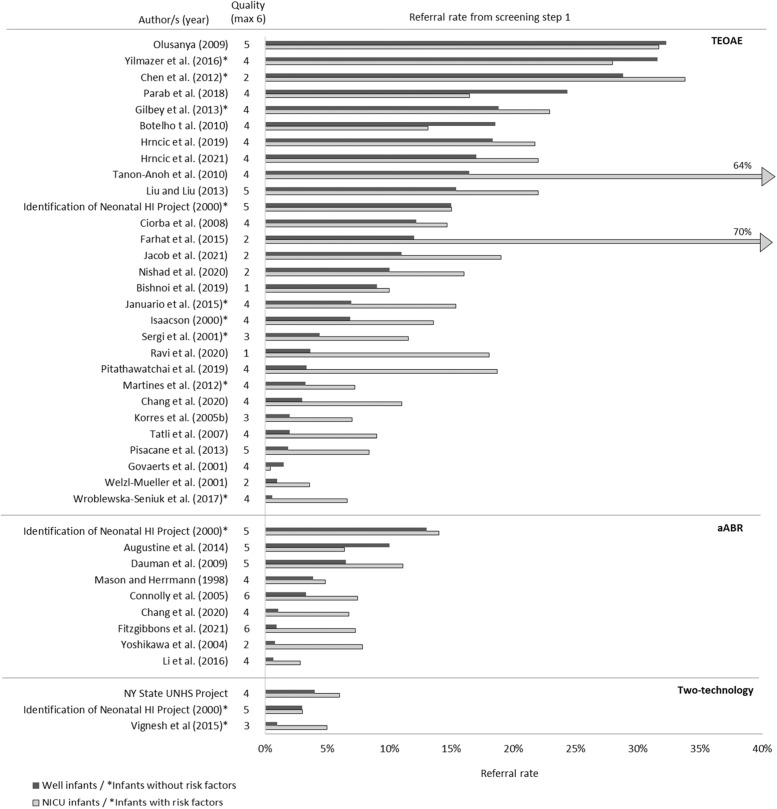
Results: Fifty-eight studies reported on referral rate, 8 on LTFU rate, and 35 on both. Only 15 studies defined LTFU. Substantial diversity in referral and LTFU rate was observed across studies. Twelve of fourteen studies that evaluated screening method showed lower referral rates with aABR compared to TEOAE for well babies (WB). Rescreening before hospital discharge and screening after 3 days of age reduced referral rates. Studies investigating LTFU reported lower rates for programmes that had audiologist involvement, did not require fees for step 2, were embedded in a larger regional or national programme, and scheduled follow-up in a location accessible to the families. In programmes with low overall LTFU, higher LTFU was observed for infants from the NICU compared to WB.
Conclusion: Although poor reporting and exclusion of non-English articles may limit the generalisability from this review, key influential factors for referral and LTFU rates were identified. Including aABR in WB screening can effectively reduce referral rates, but it is not the only solution. The reported referral and LTFU rates vary largely across studies, implying the contribution of several parameters identified in this review and the context in which the programme is performed. Extra attention should be paid to infants with higher risk for hearing impairment to ensure their return to follow-up.
Keywords: Automated auditory brainstem response; Childhood hearing impairment; Early detection and intervention; Lost to follow-up; Newborn hearing screening; Otoacoustic emissions; Quality assessment; Referral.
© 2022. The Author(s).
Conflict of interest statement
None to declare.
Figures

Similar articles
-
An effective compromise between cost and referral rate: A sequential hearing screening protocol using TEOAEs and AABRs for healthy newborns.Int J Pediatr Otorhinolaryngol. 2016 Dec;91:141-145. doi: 10.1016/j.ijporl.2016.10.025. Epub 2016 Oct 26. Int J Pediatr Otorhinolaryngol. 2016. PMID: 27863628
-
Neonatal hearing screening of high-risk infants using automated auditory brainstem response: a retrospective analysis of referral rates.Ir J Med Sci. 2014 Sep;183(3):405-10. doi: 10.1007/s11845-013-1028-5. Epub 2013 Oct 7. Ir J Med Sci. 2014. PMID: 24097063
-
When should automatic Auditory Brainstem Response test be used for newborn hearing screening?Auris Nasus Larynx. 2015 Jun;42(3):199-202. doi: 10.1016/j.anl.2014.10.005. Epub 2014 Nov 5. Auris Nasus Larynx. 2015. PMID: 25459495
-
Quality measures of two-stage newborn hearing screening: systematic review and meta-analysis.Front Public Health. 2025 Apr 16;13:1566478. doi: 10.3389/fpubh.2025.1566478. eCollection 2025. Front Public Health. 2025. PMID: 40308920 Free PMC article.
-
Otoacoustic emissions in newborn hearing screening: a systematic review of the effects of different protocols on test outcomes.Int J Pediatr Otorhinolaryngol. 2014 May;78(5):711-7. doi: 10.1016/j.ijporl.2014.01.021. Epub 2014 Jan 27. Int J Pediatr Otorhinolaryngol. 2014. PMID: 24613088
Cited by
-
Community-based infant hearing screening: Outcomes of a rural pilot programme.S Afr J Commun Disord. 2024 Oct 31;71(1):e1-e8. doi: 10.4102/sajcd.v71i1.1045. S Afr J Commun Disord. 2024. PMID: 39494639 Free PMC article.
-
Neonatal hearing screening - does failure in TEOAE screening matter when the AABR test is passed?Eur Arch Otorhinolaryngol. 2024 Mar;281(3):1273-1283. doi: 10.1007/s00405-023-08250-z. Epub 2023 Oct 13. Eur Arch Otorhinolaryngol. 2024. PMID: 37831131 Free PMC article.
-
Implementation of Newborn Hearing Screening in Albania.Int J Neonatal Screen. 2023 May 10;9(2):28. doi: 10.3390/ijns9020028. Int J Neonatal Screen. 2023. PMID: 37218893 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
