

Budget impact analysis of a multifaceted nurse-led intervention to reduce indwelling urinary catheter use in New South Wales Hospitals
- PMID: 35932078
- PMCID: PMC9356439
- DOI: 10.1186/s12913-022-08313-7
Budget impact analysis of a multifaceted nurse-led intervention to reduce indwelling urinary catheter use in New South Wales Hospitals
Abstract
Background: In hospitals, catheter acquired urinary tract infection causes significant resource waste and discomfort among admitted patients. An intervention for reducing indwelling catheterisations - No-CAUTI - was trialled across four hospitals in New South Wales, Australia. No-CAUTI includes: train-the-trainer workshops, site champions, compliance audits, and point prevalence surveys. The trial showed reductions on usual care catheterisation rates at 4- and 9-month post-intervention. This result was statistically non-significant; and post-intervention catheterisation rates rebounded between 4 and 9 months. However, No-CAUTI showed statistically significant catheterisation decreases for medical wards, female patients and for short-term catheterisations. This study presents a budget impact analysis of a projected five year No-CAUTI roll out across New South Wales public hospitals, from the cost perspective of the New South Wales Ministry of Health.
Methods: Budget forecasts were made for five year roll outs of: i) No-CAUTI; and ii) usual care, among all public hospitals in New South Wales hosting overnight stays (n=180). The roll out design maintains intervention effectiveness with ongoing workshops, quality audits, and hospital surveys. Forecasts of catheterisations, procedures and treatments were modelled on No-CAUTI trial observations. Costs were sourced from trial records, the Medical Benefits Scheme, the Pharmaceutical Benefits Scheme and public wage awards. Cost and parameter uncertainties were considered with sensitivity scenarios.
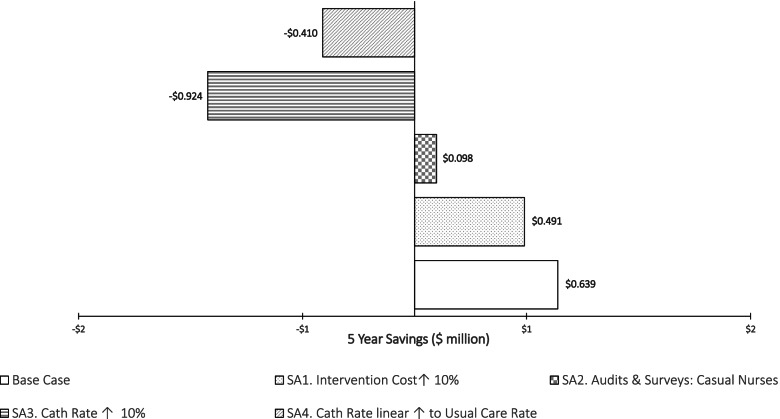
Results: The estimated five-year No-CAUTI roll-out cost was $1.5 million. It had an overall budget saving of $640,000 due to reductions of 100,100 catheterisations, 33,300 urine tests and 6,700 antibiotics administrations. Non-Metropolitan hospitals had a net saving of $1.2 million, while Metropolitan hospitals had a net cost of $0.54 million.
Conclusions: Compared to usual care, NO-CAUTI is expected to realise overall budget savings and decreases in catheterisations over five years. These findings allow a consideration of the affordability of a wide implementation.
Trial registration: Registered with the Australian New Zealand Clinical Trials Registry ( ACTRN12617000090314 ). First registered 17 January 2017, retrospectively. First enrolment, 15/11/2016.
Keywords: Budget Impact Analysis; Catheters; Nurses; Urinary Tract Infections.
© 2022. The Author(s).
Conflict of interest statement
All authors have completed the unified completing interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Duckett SJ, Breadon P, Weidmann B, Nicola I. Controlling costly care: a billiondollar hospital opportunity. Melbourne: Grattan Institute; 2014.
-
- Productivity Commission. Efficiency in Health. Commission Research Paper. Canberra: Productivity Commission. 2015.
-
- Searles A, Gleeson M, Reeves P, Jorm C, Leeder S, Karnon J, Hiscock H, Skouteris H, Daly M. The Local Level Evaluation of Healthcare in Australia, Health Systems Improvement and Sustainability (HSIS) National Initiative. Newcastle: NSW Regional Health Partners; 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
