

Trans-Posterior Cruciate Ligament All-Inside Root Repair Versus Partial Meniscectomy for Medial Meniscus Posterior Root Tears: Comparison of Semiquantitative and Quantitative MRI Outcomes in Cartilage Degeneration and Osteoarthritic Progression
- PMID: 35932104
- PMCID: PMC9364209
- DOI: 10.1177/19476035221114242
Trans-Posterior Cruciate Ligament All-Inside Root Repair Versus Partial Meniscectomy for Medial Meniscus Posterior Root Tears: Comparison of Semiquantitative and Quantitative MRI Outcomes in Cartilage Degeneration and Osteoarthritic Progression
Abstract
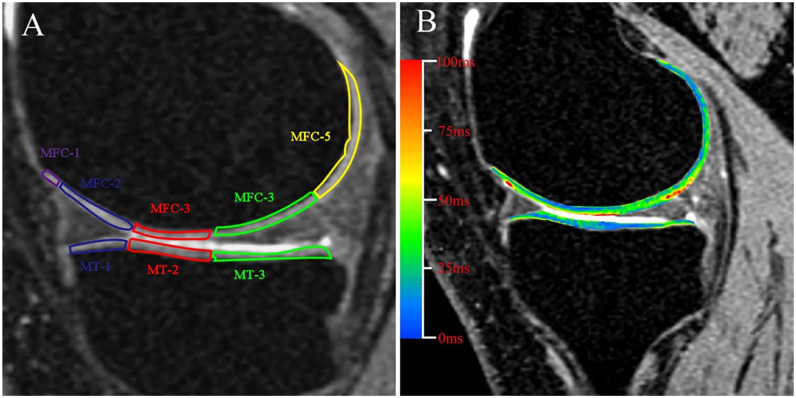
Objective: To perform conventional, morphological, and T2 mapping compositional MRI imaging to assess the cartilage degeneration and osteoarthritic progression in patients with medial meniscus posterior root tears (MMPRTs) who underwent trans-posterior cruciate ligament (PCL) all-inside repair or partial meniscectomy.
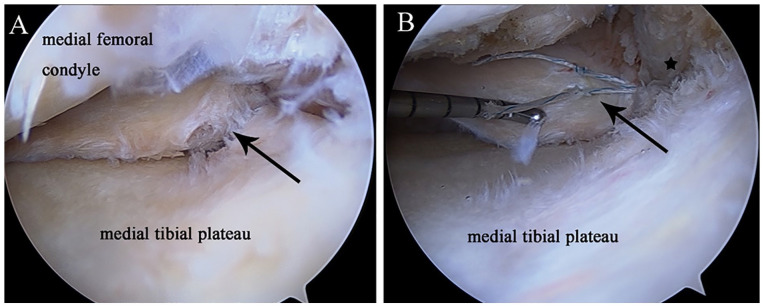
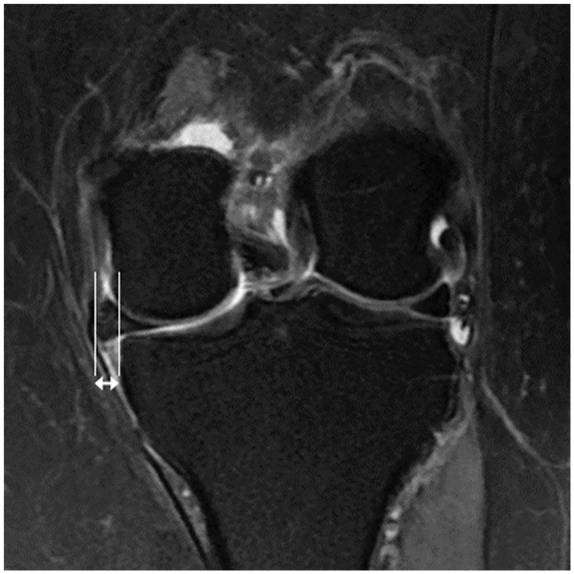
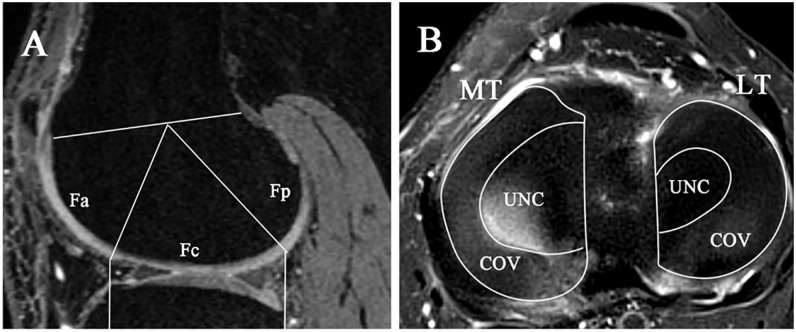
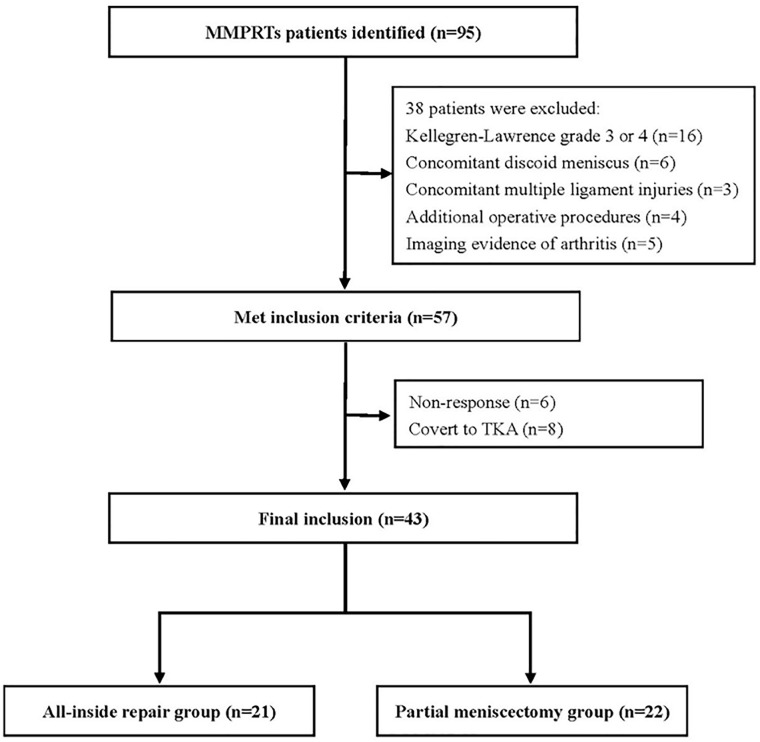
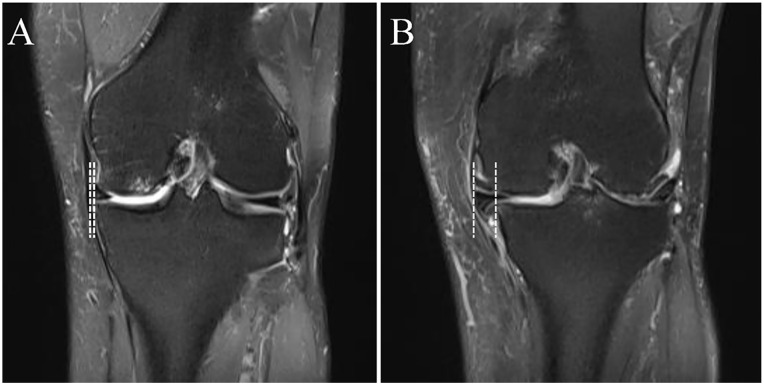
Design: Patients with MMPRTs after trans-PCL all-inside repair (group AR) or partial meniscectomy (group PM) between 2015 and 2018 were retrospectively identified. Preoperative and postoperative conventional MRI were collected to assess medial meniscus extrusion (MME) and the whole-organ magnetic resonance imaging score (WORMS). Postoperative morphological MRI and T2 mapping compositional MRI were collected to evaluate the quantitative cartilage thickness/volume and cartilage composition.
Results: The final cohort consisted of 21 patients in group AR and 22 patients in group PM, with no differences in demographic data and baseline patient characteristics between the 2 groups. Group AR demonstrated less progression of articular cartilage wear (P < 0.05) and decreased meniscal extrusion (P = 0.008) than group PM at the final follow-up. In addition, group AR demonstrated less extracellular matrix degeneration in the cartilage subregion of the medial compartment (P < 0.05) than group PM with lower T2 relaxation times in the superficial layer of the articular cartilage.
Conclusion: Trans-PCL all-inside repair of MMPRTs could delay the initial cartilage deterioration and morphological cartilage degeneration compared with partial meniscectomy. However, the amount of residual meniscal extrusion is clinically important, and an improved root repair fixation method should be investigated.
Keywords: MRI evaluation; all-inside repair; medial meniscus; meniscus root tear.
Conflict of interest statement
Figures
Similar articles
-
Clinical, Radiographic, and MRI Evaluation of All-Inside Medial Meniscus Posterior Root Repair via Suture Fixation to the Posterior Cruciate Ligament Versus Partial Meniscectomy: Results at 3-Year Follow-up.Orthop J Sports Med. 2023 Jul 7;11(7):23259671231180545. doi: 10.1177/23259671231180545. eCollection 2023 Jul. Orthop J Sports Med. 2023. PMID: 37435421 Free PMC article.
-
High-resolution magnetic resonance imaging can predict osteoarthritic progression after medial meniscus posterior root injury: randomized in vivo experimental study in a rabbit model.J ISAKOS. 2024 Aug;9(4):526-533. doi: 10.1016/j.jisako.2024.03.015. Epub 2024 Apr 5. J ISAKOS. 2024. PMID: 38583525
-
Non-anatomic repair of medial meniscus posterior root tears to the posterior capsule provided favourable outcomes in middle-aged and older patients.Knee Surg Sports Traumatol Arthrosc. 2021 Dec;29(12):4261-4269. doi: 10.1007/s00167-021-06532-9. Epub 2021 Apr 9. Knee Surg Sports Traumatol Arthrosc. 2021. PMID: 33835225
-
Comparison of Long-term Radiographic Outcomes and Rate and Time for Conversion to Total Knee Arthroplasty Between Repair and Meniscectomy for Medial Meniscus Posterior Root Tears: A Systematic Review and Meta-analysis.Am J Sports Med. 2022 Jun;50(7):2023-2031. doi: 10.1177/03635465211017514. Epub 2021 Jul 12. Am J Sports Med. 2022. PMID: 34251898
-
Surgical treatment of complex meniscus tear and disease: state of the art.J ISAKOS. 2021 Jan;6(1):35-45. doi: 10.1136/jisakos-2019-000380. Epub 2020 Sep 17. J ISAKOS. 2021. PMID: 33833044 Review.
Cited by
-
Osteoarthritis Development Following Meniscectomy vs. Meniscal Repair for Posterior Medial Meniscus Injuries: A Systematic Review.Medicina (Kaunas). 2024 Mar 30;60(4):569. doi: 10.3390/medicina60040569. Medicina (Kaunas). 2024. PMID: 38674215 Free PMC article.
-
Younger patients, lower BMI, complete meniscus root healing, lower HKA degree and shorter preoperative symptom duration were the independent risk factors correlated with the good correction of MME in patients with repaired MMPRTs.Knee Surg Sports Traumatol Arthrosc. 2023 Sep;31(9):3775-3783. doi: 10.1007/s00167-023-07330-1. Epub 2023 Feb 15. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 36790456
-
Diagnosis and Treatment Strategies of Meniscus Root Tears: A Scoping Review.Orthop J Sports Med. 2024 Nov 1;12(11):23259671241283962. doi: 10.1177/23259671241283962. eCollection 2024 Nov. Orthop J Sports Med. 2024. PMID: 39493310 Free PMC article.
-
Meniscectomy is associated with a higher rate of osteoarthritis compared to meniscal repair following acute tears: a meta-analysis.Knee Surg Sports Traumatol Arthrosc. 2023 Dec;31(12):5485-5495. doi: 10.1007/s00167-023-07600-y. Epub 2023 Oct 9. Knee Surg Sports Traumatol Arthrosc. 2023. PMID: 37812251 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
