

Epidemiology, risk factors, and outcomes of lung retransplantation: An analysis of the International Society for Heart and Lung Transplantation Thoracic Transplant Registry
- PMID: 35933297
- PMCID: PMC9986966
- DOI: 10.1016/j.healun.2022.06.022
Epidemiology, risk factors, and outcomes of lung retransplantation: An analysis of the International Society for Heart and Lung Transplantation Thoracic Transplant Registry
Abstract
Background: Lung retransplantation is a complex surgical decision that represents the only potential treatment option for recipients suffering from lung allograft failure. We sought to describe the modern landscape of lung retransplantation and to compare the relative importance of selected clinical, donor, and recipient factors on mortality in the year following lung retransplantation.
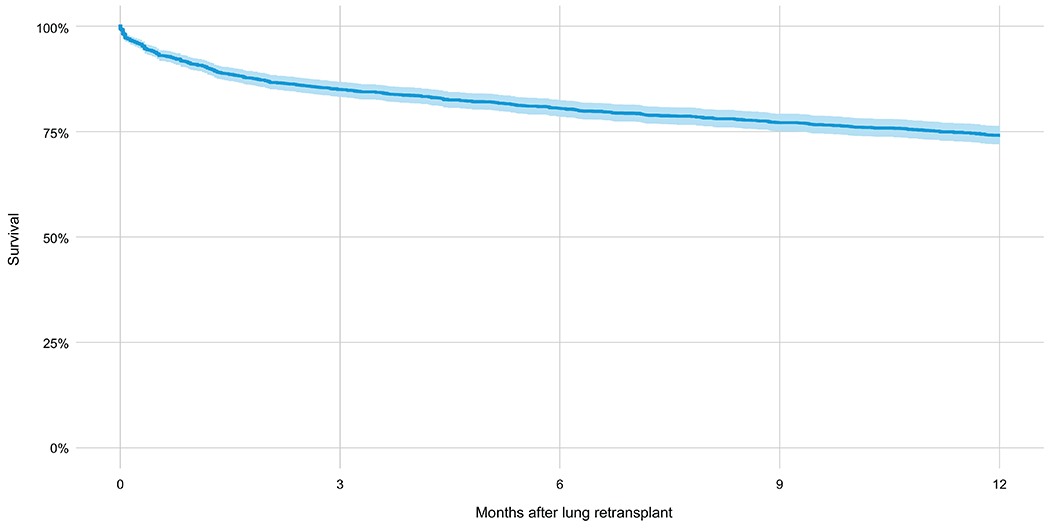
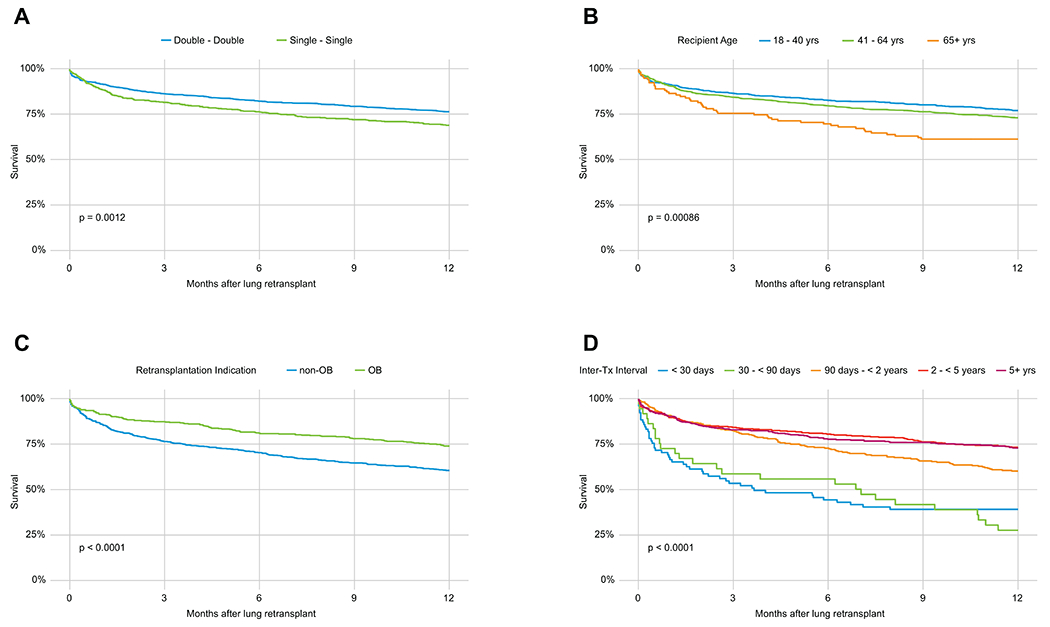
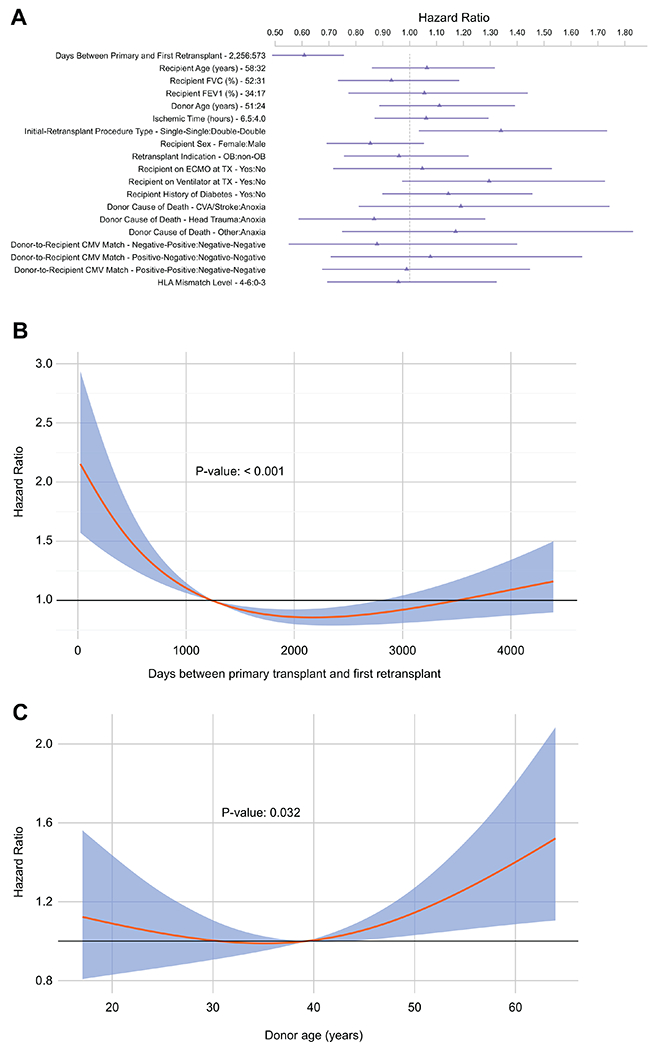
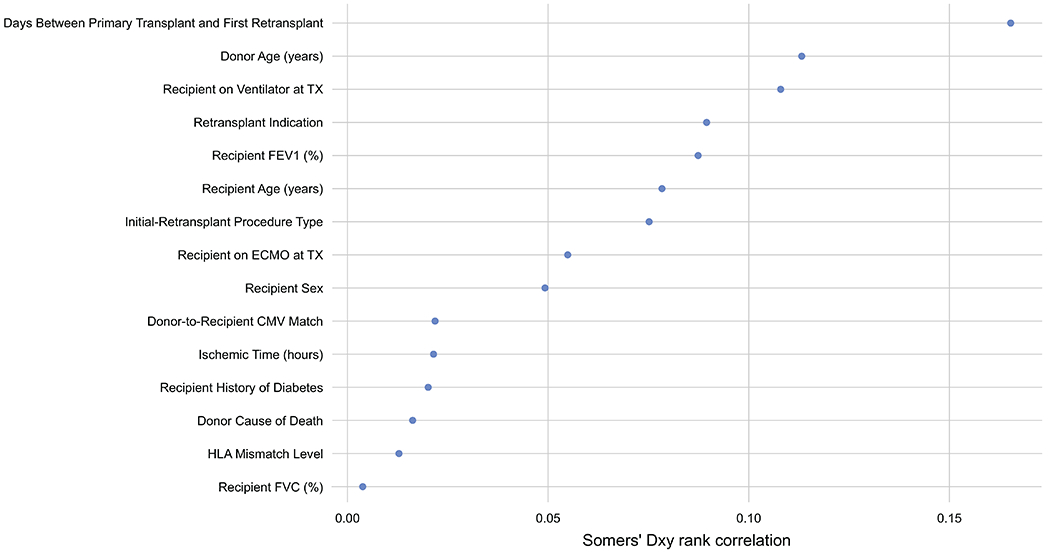
Methods: We conducted a retrospective cohort study of first-time adult recipients of deceased donor lung retransplants reported to the International Society for Heart and Lung Transplantation (ISHLT) Thoracic Transplant Registry from May 2005 through June 2017. In addition to describing the characteristics of lung retransplant recipients, we examined 1 year survival overall, and by initial transplant-retransplant procedure type, recipient age, retransplant indication, and time-to-lung retransplantation (i.e., inter-transplant interval). We used the Somers' Dxy rank correlation statistic for censored data to assess the relative importance of several potential prognostic risk factors for mortality in the year following lung retransplantation.
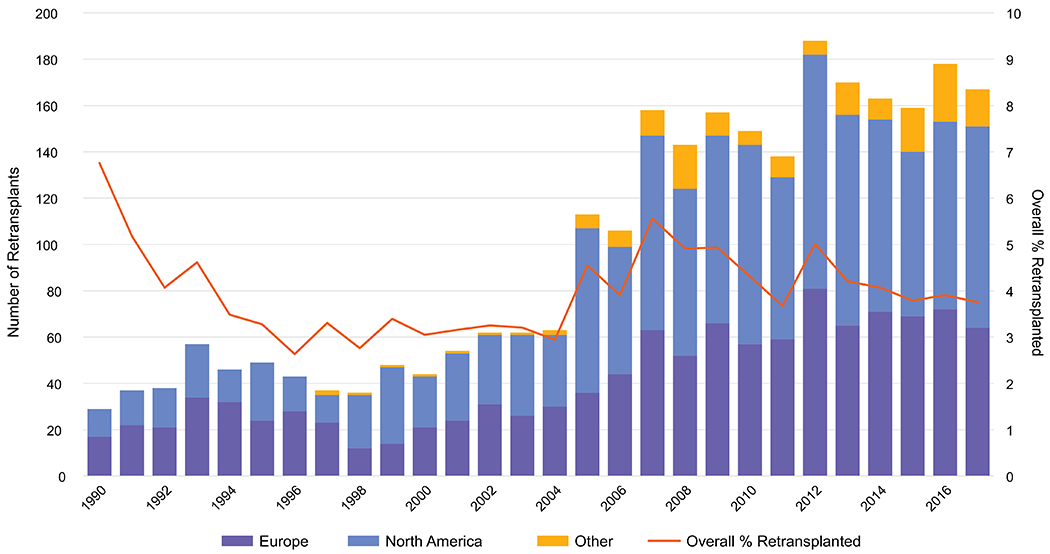
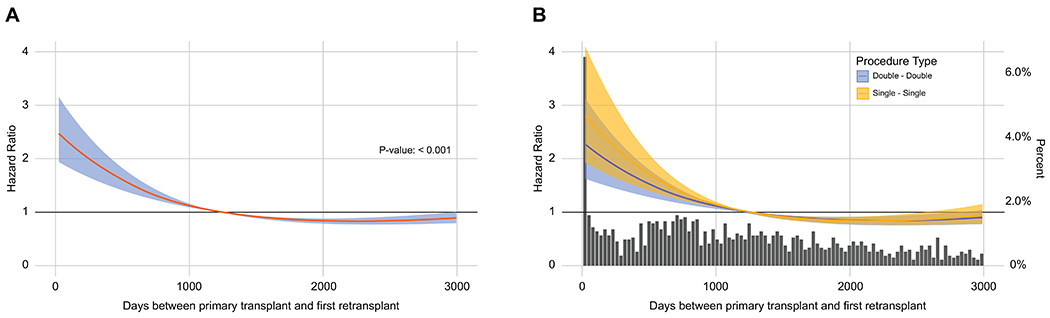
Results: Our cohort included 1,597 lung retransplant recipients. 2005 was the first year with more than 100 retransplants, and since 2007, 138 to 188 retransplants (approximately 4%-6% of all transplants) were reported annually to the ISHLT Registry. The median inter-transplant interval was 3.4 years (interquartile range: 1.6-6.2 years). Forty-three percent of the cohort had an obliterative bronchiolitis retransplant indication, whereas 17% had primary graft failure. One-third (32%) were retransplanted within 2 years of their primary transplant, and 64% received a double lung transplant both times, whereas 36% received consecutive single lung transplants. Six-month and 1 year survival (82% and 76%) were higher for double-double lung retransplant recipients than for single-single recipients (76% and 69%). The 3 strongest prognostic factors for 1 year mortality were the inter-transplant interval (decreasing hazard with longer intervals), donor age (increasing hazard with older age), and need for mechanical ventilation preceding lung retransplantation.
Conclusions: Retransplants comprise approximately 5% of annual lung transplants worldwide. The factor most strongly associated with 1 year mortality in this population was the duration of time since the primary lung transplant, with a persistent reduction in risk as more time elapses.
Keywords: allograft failure; end-stage lung disease; epidemiology; lung transplant; retransplantation.
Copyright © 2022 International Society for Heart and Lung Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Mortality and morbidity after retransplantation after primary heart transplant in childhood: an analysis from the registry of the International Society for Heart and Lung Transplantation.J Heart Lung Transplant. 2014 Mar;33(3):241-51. doi: 10.1016/j.healun.2013.11.006. Epub 2013 Nov 28. J Heart Lung Transplant. 2014. PMID: 24462559
-
Thoracic retransplantation: Does time to retransplantation matter?J Thorac Cardiovasc Surg. 2023 Dec;166(6):1529-1541.e4. doi: 10.1016/j.jtcvs.2022.05.003. Epub 2022 May 15. J Thorac Cardiovasc Surg. 2023. PMID: 36049964
-
The Optimal Procedure for Retransplantation After Single Lung Transplantation.Ann Thorac Surg. 2017 Jul;104(1):170-175. doi: 10.1016/j.athoracsur.2016.10.002. Epub 2017 Jan 18. Ann Thorac Surg. 2017. PMID: 28109573
-
Cardiac retransplantation in children.Ann Thorac Surg. 2004 Aug;78(2):644-9; discussion 644-9. doi: 10.1016/j.athoracsur.2004.02.090. Ann Thorac Surg. 2004. PMID: 15276538 Review.
-
Retransplantation following isolated lung transplantation.Semin Thorac Cardiovasc Surg. 1992 Apr;4(2):122-5. Semin Thorac Cardiovasc Surg. 1992. PMID: 1627691 Review.
Cited by
-
Worth a Double Take? An In-Depth Review of Lung Retransplantation.J Clin Med. 2023 Nov 30;12(23):7418. doi: 10.3390/jcm12237418. J Clin Med. 2023. PMID: 38068470 Free PMC article. Review.
-
Incidence of malignancies after lung transplantation and their effect on the outcome. 26 years' experience.Heliyon. 2023 Sep 30;9(10):e20592. doi: 10.1016/j.heliyon.2023.e20592. eCollection 2023 Oct. Heliyon. 2023. PMID: 37810874 Free PMC article.
-
Effect of chronic lung allograft dysfunction phenotypes on the outcome after lung retransplantation: A retrospective single-center data analysis.JTCVS Open. 2024 Nov 19;23:335-348. doi: 10.1016/j.xjon.2024.10.034. eCollection 2025 Feb. JTCVS Open. 2024. PMID: 40061536 Free PMC article.
-
Significantly reduced patient and graft survival for left vs right donor lungs for lung transplant recipients.JHLT Open. 2024 Aug 21;6:100148. doi: 10.1016/j.jhlto.2024.100148. eCollection 2024 Nov. JHLT Open. 2024. PMID: 40145044 Free PMC article.
-
Survival of patients with advanced chronic lung allograft dysfunction and the role of redo transplantation.JHLT Open. 2025 Mar 27;8:100257. doi: 10.1016/j.jhlto.2025.100257. eCollection 2025 May. JHLT Open. 2025. PMID: 40491547 Free PMC article.
References
-
- Seiler A, Klaghofer R, Ture M, Komossa K, Martin-Soelch C, Jenewein J: A systematic review of health-related quality of life and psychological outcomes after lung transplantation. J Heart Lung Transplant 2016;35:195–202. - PubMed
-
- Rana A, Gruessner A, Agopian VG, et al.: Survival benefit of solid-organ transplant in the United States. JAMA Surg 2015;150:252–9. - PubMed
-
- Verleden GM, Glanville AR, Lease ED, et al.: Chronic lung allograft dysfunction: Definition, diagnostic criteria, and approaches to treatment-A consensus report from the Pulmonary Council of the ISHLT. J Heart Lung Transplant 2019;38:493–503. - PubMed
-
- Strueber M, Fischer S, Gottlieb J, et al.: Long-term outcome after pulmonary retransplantation. J Thorac Cardiovasc Surg 2006;132:407–12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
