

Comparison of nutritional risk status assessment tools in predicting 30-day survival in critically ill COVID-19 pneumonia patients
- PMID: 35933605
- PMCID: PMC9357296
- DOI: 10.5144/0256-4947.2022.236
Comparison of nutritional risk status assessment tools in predicting 30-day survival in critically ill COVID-19 pneumonia patients
Abstract
Background: Few clinical studies have addressed nutritional risk assessment in patients with COVID-19 pneumonia admitted to the intensive care unit (ICU).
Objectives: Assess the nutritional risk status of the critically ill COVID-19 pneumonia patients admitted to the ICU, and compare the nutritional risk screening tools.
Design: Medical record review SETTING: Tertiary critical care unit PATIENTS AND METHODS: We included adult (age >18 years) PCR-confirmed critically ill COVID-19 pneumonia cases admitted to the ICU between August 2020 and September 2021. Scoring systems were used to assess COVID-19 severity and nutritional status (mNUTRIC: modified Nutrition Risk in Critically Ill, NRS2002: Nutritional Risk Screening 2002). The 30-day mortality prediction performance of nutritional scores and survival comparisons between clinical and demographic factors were assessed.
Main outcome measures: Compare the nutrition risk tools SAMPLE SIZE: 281 patients with a mean (SD) age of 64.3 (13.3) years; 143 (50.8%) were 65 years and older.
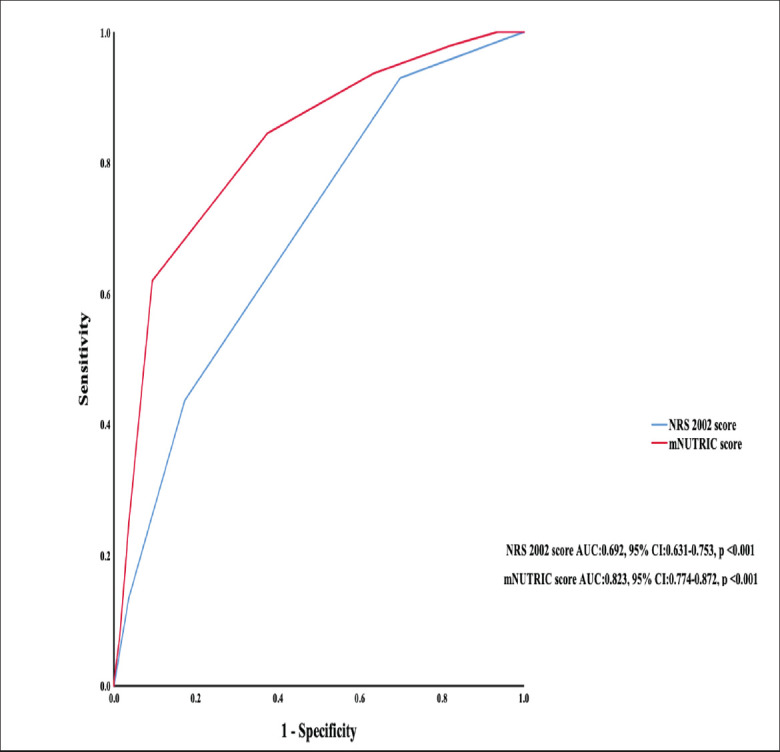
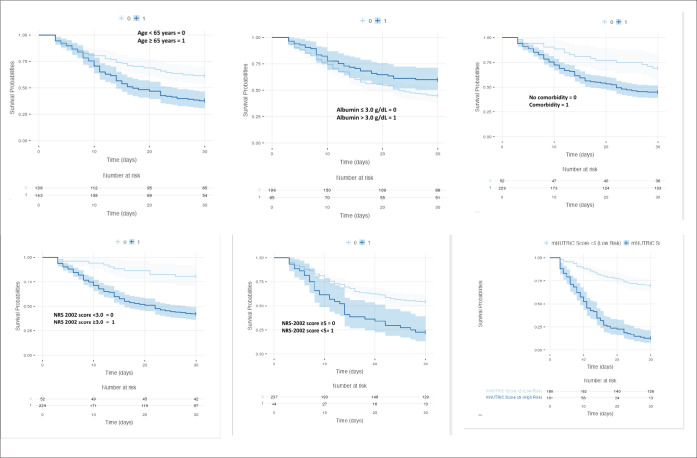
Results: The mean mNUTRIC score of the cases was 3.81 (1.66) and the mean NRS-2002 score was 3.21 (0.84.), and 101 (35.9%) were at high risk of malnutrition according to the mNUTRIC score and 229 (81.4%) according to the NRS 2002 score. In cases at high risk of malnutrition by the mNUTRIC score there was a greater need for invasive mechanical ventilation, vasopressors, and renal replacement therapy (P<.001 for all comparisons). The mNUTRIC score was superior to the NRS-2002 score in estimating 30-day mortality. In patients who died within 30 days, the mNUTRIC score and NRS-2002 score on the day of hospitalization were significantly higher (P<.001), and the proportion of patients with NRS-2002 score ≥3 and mNUTRIC score ≥5 was significantly higher in the non-surviving group (P<.001). In addition, patients with a high risk of malnutrition had a shorter survival time. The mNUTRIC score was an independent and important prognostic factor for 30-day mortality, and patients with an mNUTRIC score ≥5 had a 6.26-fold risk for 30-day mortality in the multivariate Cox regression.
Conclusion: One third of critical COVID-19 pneumonia cases hospitalized in the ICU due to acute respiratory failure have a high risk of malnutrition, and a high mNUTRIC score is associated with increased mortality.
Limitations: Single center retrospective study.
Conflict of interest: None.
Figures
Similar articles
-
The modified NUTRIC score can be used for nutritional risk assessment as well as prognosis prediction in critically ill COVID-19 patients.Clin Nutr. 2021 Feb;40(2):534-541. doi: 10.1016/j.clnu.2020.05.051. Epub 2020 Jun 5. Clin Nutr. 2021. PMID: 32527576 Free PMC article.
-
The modified NUTRIC score (mNUTRIC) is associated with increased 28-day mortality in critically ill COVID-19 patients: Internal validation of a prediction model.Clin Nutr ESPEN. 2022 Apr;48:202-209. doi: 10.1016/j.clnesp.2022.02.014. Epub 2022 Feb 17. Clin Nutr ESPEN. 2022. PMID: 35331492 Free PMC article.
-
NUTRIC Score: Isolated and Combined Use With the NRS-2002 to Predict Hospital Mortality in Critically Ill Patients.JPEN J Parenter Enteral Nutr. 2020 Sep;44(7):1250-1256. doi: 10.1002/jpen.1804. Epub 2020 Feb 6. JPEN J Parenter Enteral Nutr. 2020. PMID: 32026516
-
Nutritional risk in critically ill patients: how it is assessed, its prevalence and prognostic value: a systematic review.Nutr Rev. 2020 Dec 1;78(12):1052-1068. doi: 10.1093/nutrit/nuaa031. Nutr Rev. 2020. PMID: 32529226
-
Nutritional Risk Screening Tools for Older Adults with COVID-19: A Systematic Review.Nutrients. 2020 Sep 27;12(10):2956. doi: 10.3390/nu12102956. Nutrients. 2020. PMID: 32992538 Free PMC article.
Cited by
-
A Novel Facet of In-Hospital Food Consumption Associated with Hospital Mortality in Patients with Scheduled Admission-Addition of a Study Protocol to Test the Existence of Effects of COVID-19 in the Same Study in the Post-COVID-19 Period.Nutrients. 2024 Jul 19;16(14):2327. doi: 10.3390/nu16142327. Nutrients. 2024. PMID: 39064770 Free PMC article.
-
The association between nutrition risk status assessment and hospital mortality in Chinese older inpatients: a retrospective study.J Health Popul Nutr. 2024 Dec 27;43(1):229. doi: 10.1186/s41043-024-00726-w. J Health Popul Nutr. 2024. PMID: 39731201 Free PMC article.
-
Systematic Review and Meta-Analysis: Malnutrition and In-Hospital Death in Adults Hospitalized with COVID-19.Nutrients. 2023 Mar 6;15(5):1298. doi: 10.3390/nu15051298. Nutrients. 2023. PMID: 36904295 Free PMC article.
-
The Impact of the COVID-19 Pandemic in the Interrelationships Among Mental Health, Nutritional Status and Lifestyle Factors of Older Adults: A Cross-Sectional Study in the Pre- and Post-Covid Periods.Nutrients. 2025 Jan 10;17(2):249. doi: 10.3390/nu17020249. Nutrients. 2025. PMID: 39861378 Free PMC article.
References
-
- Xu W, Sun NN, Gao HN, Chen ZY, Yang Y, Ju B, et al. . Risk factors analysis of COVID-19 patients with ARDS and prediction based on machine learning. Sci Rep. 2021;11(1):2933. Epub 2021/02/05. doi: 10.1038/s41598-021-82492-x. PubMed PMID: 33536460; PubMed Central PMCID: PMC7858607. - DOI - PMC - PubMed
-
- Odabasi Z, Cinel I. Consideration of Severe Coronavirus Disease 2019 As Viral Sepsis and Potential Use of Immune Checkpoint Inhibitors. Crit Care Explor. 2020;2(6):e0141. Epub 2020/07/23. doi: 10.1097/CCE.0000000000000141. PubMed PMID: 32696004; PubMed Central PMCID: PMC7314326. - DOI - PMC - PubMed
-
- Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J Heart Lung Transplant. 2020;39(5):405–7. Epub 2020/05/05. doi: 10.1016/j.healun.2020.03.012. PubMed PMID: 32362390; PubMed Central PMCID: PMC7118652. - DOI - PMC - PubMed
-
- Loi M, Wang J, Ong C, Lee JH. Nutritional support of critically ill adults and children with acute respiratory distress syndrome: A clinical review. Clinical Nutrition ESPEN. 2017;19:1–8. doi: 10.1016/j.clnesp.2017.02.005. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials