

Clinical Experience with "Stand-Alone" Elephant Trunk Procedure for Descending Aortic Aneurysms
- PMID: 35933985
- PMCID: PMC9357495
- DOI: 10.1055/s-0042-1743535
Clinical Experience with "Stand-Alone" Elephant Trunk Procedure for Descending Aortic Aneurysms
Abstract
Background: Both open and endovascular treatments of descending thoracic aortic aneurysms require a secure proximal landing zone. This may be difficult to achieve when the dilatation extends proximally to the left subclavian level. Clamping above the aneurysm may be difficult. In the case of an endovascular approach, achieving a suitable landing zone may require extensive extra-anatomic debranching, which is not without complications and limitations.
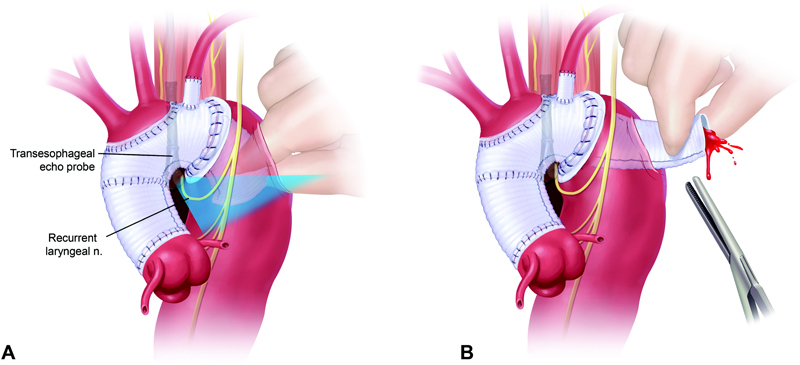
Methods: We describe a modification of the traditional elephant trunk procedure that represents a "stand-alone" elephant trunk. Under deep hypothermic circulatory arrest, the aorta is transected between the left carotid and left subclavian arteries. A simple, noninverted elephant trunk is placed through the distal cut aorta. The two ends are sewn back together, incorporating the lip of the elephant trunk in the anastomosis. We review our experience in five patients who underwent this procedure.
Results: All 5 patients (4 males, 1 female) aged 41 to 68 (mean, 57 years) tolerated the Stage 1 stand-alone elephant trunk procedure well, without mortality, stroke, or bleeding. The Stage 2 descending aortic replacements were performed at a mean of 6.7 months after Stage 1. There was no Stage 2 mortality, stroke, or bleeding. One patient died 8 years later of cardiac cause, and the remaining are alive and well.
Conclusion: A stand-alone elephant trunk procedure is safe and straightforward and provides an excellent proximal foundation for subsequent open (or potentially endovascular) descending aortic replacement.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. (https://creativecommons.org/licenses/by/4.0/).
Conflict of interest statement
Dr. Elefteriades is Principal of CoolSpine, member of Data and Safety Monitoring Board for Terumo, and Consultant for CryoLife. The remaining authors do not declare any conflict of interest related to this article.
Figures

References
-
- Svensson L G. The elephant trunk procedure: uses in complex aortic diseases. Curr Opin Cardiol. 2005;20(06):491–495. - PubMed
-
- Roselli E E, Subramanian S, Sun Z.Endovascular versus open elephant trunk completion for extensive aortic disease J Thorac Cardiovasc Surg 2013146061408–1416., discussion 1416–1417 - PubMed
-
- Abdelbaky M, Zafar M A, Saeyeldin A. Routine anterior spinal artery visualization prior to descending and thoracoabdominal aneurysm repair: high detection success. J Card Surg. 2019;34(12):1563–1568. - PubMed
-
- Crawford E S, Coselli J S, Svensson L G, Safi H J, Hess K R. Diffuse aneurysmal disease (chronic aortic dissection, Marfan, and mega aorta syndromes) and multiple aneurysm. Treatment by subtotal and total aortic replacement emphasizing the elephant trunk operation. Ann Surg. 1990;211(05):521–537. - PMC - PubMed
LinkOut - more resources
Full Text Sources