

Low-dose intravenous plus inhaled versus intravenous polymyxin B for the treatment of extensive drug-resistant Gram-negative ventilator-associated pneumonia in the critical illnesses: a multi-center matched case-control study
- PMID: 35934730
- PMCID: PMC9357592
- DOI: 10.1186/s13613-022-01033-5
Low-dose intravenous plus inhaled versus intravenous polymyxin B for the treatment of extensive drug-resistant Gram-negative ventilator-associated pneumonia in the critical illnesses: a multi-center matched case-control study
Abstract
Background: The mortality of extensively drug-resistant Gram-negative (XDR GN) bacilli-induced ventilator-associated pneumonia (VAP) is extremely high. The purpose of this study was to compare the efficacy and safety of inhaled (IH) plus intravenous (IV) polymyxin B versus IV polymyxin B in XDR GN bacilli VAP patients.
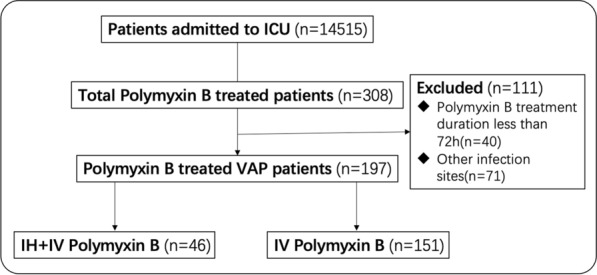
Methods: A retrospective multi-center observational cohort study was performed at eight ICUs between January 1st 2018, and January 1st 2020 in China. Data from all patients treated with polymyxin B for a microbiologically confirmed VAP were analyzed. The primary endpoint was the clinical cure of VAP. The favorable clinical outcome, microbiological outcome, VAP-related mortality and all-cause mortality during hospitalization, and side effects related with polymyxin B were secondary endpoints. Favorable clinical outcome included clinical cure or clinical improvement.
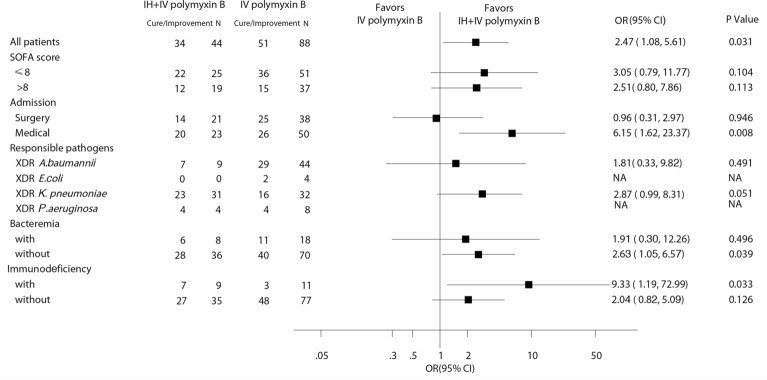
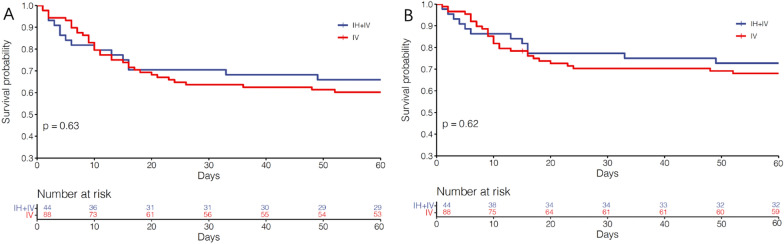
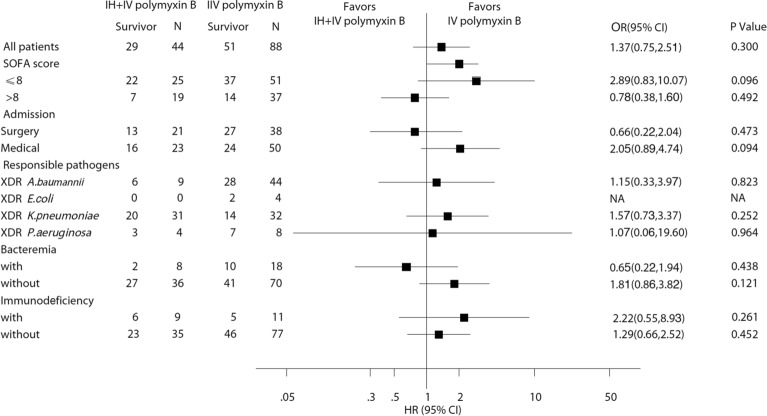
Results: 151 patients and 46 patients were treated with IV polymyxin B and IH plus IV polymyxin B, respectively. XDR Klebsiella pneumoniae was the main isolated pathogen (n = 83, 42.1%). After matching on age (± 5 years), gender, septic shock, and Apache II score (± 4 points) when polymyxin B was started, 132 patients were included. 44 patients received simultaneous IH plus IV polymyxin B and 88 patients received IV polymyxin B. The rates of clinical cure (43.2% vs 27.3%, p = 0.066), bacterial eradication (36.4% vs 23.9%, p = 0.132) as well as VAP-related mortality (27.3% vs 34.1%, p = 0.428), all-cause mortality (34.1% vs 42.0%, p = 0.378) did not show any significant difference between the two groups. However, IH plus IV polymyxin B therapy was associated with improved favorable clinical outcome (77.3% vs 58.0%, p = 0.029). Patients in the different subgroups (admitted with medical etiology, infected with XDR K. pneumoniae, without bacteremia, with immunosuppressive status) were with odd ratios (ORs) in favor of the combined therapy. No patient required polymyxin B discontinuation due to adverse events. Additional use of IH polymyxin B (aOR 2.63, 95% CI 1.06, 6.66, p = 0.037) was an independent factor associated with favorable clinical outcome.
Conclusions: The addition of low-dose IH polymyxin B to low-dose IV polymyxin B did not provide efficient clinical cure and bacterial eradication in VAP caused by XDR GN bacilli. Keypoints Additional use of IH polymyxin B was the sole independent risk factor of favorable clinical outcome. Patients in the different subgroups were with HRs substantially favoring additional use of IH polymyxin B. No patients required polymyxin B discontinuation due to adverse events.
Keywords: Critical illnesses; Extensively drug-resistant Gram-negative bacilli; Inhalation; Polymyxin B; Ventilator-associated pneumonia.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interest.
Figures
Similar articles
-
Use of polymyxin B with different administration methods in the critically ill patients with ventilation associated pneumonia: a single-center experience.Front Pharmacol. 2023 Sep 1;14:1222044. doi: 10.3389/fphar.2023.1222044. eCollection 2023. Front Pharmacol. 2023. PMID: 37719858 Free PMC article.
-
Inhaled alone versus inhaled plus intravenous polymyxin B for the treatment of pneumonia due to carbapenem-resistant gram-negative bacteria: A prospective randomized controlled trial.Int J Antimicrob Agents. 2025 May;65(5):107483. doi: 10.1016/j.ijantimicag.2025.107483. Epub 2025 Feb 27. Int J Antimicrob Agents. 2025. PMID: 40023452 Clinical Trial.
-
Comparison of the clinical efficacy and toxicity of nebulized polymyxin monotherapy and combined intravenous and nebulized polymyxin for the treatment of ventilator-associated pneumonia caused by carbapenem-resistant gram-negative bacteria: a retrospective cohort study.Front Pharmacol. 2023 Aug 16;14:1209063. doi: 10.3389/fphar.2023.1209063. eCollection 2023. Front Pharmacol. 2023. PMID: 37663252 Free PMC article.
-
Cefiderocol: A Siderophore Cephalosporin with Activity Against Carbapenem-Resistant and Multidrug-Resistant Gram-Negative Bacilli.Drugs. 2019 Feb;79(3):271-289. doi: 10.1007/s40265-019-1055-2. Drugs. 2019. PMID: 30712199 Review.
-
Clinical use of intravenous polymyxin B for the treatment of patients with multidrug-resistant Gram-negative bacterial infections: An evaluation of the current evidence.J Glob Antimicrob Resist. 2021 Mar;24:342-359. doi: 10.1016/j.jgar.2020.12.026. Epub 2021 Jan 21. J Glob Antimicrob Resist. 2021. PMID: 33486122 Review.
Cited by
-
Clinical outcomes and safety of polymyxin B versus tigecycline combination therapy for pneumonia of carbapenem-resistant Klebsiella pneumoniae: a retrospective cohort study.Ann Med. 2024 Dec;56(1):2397087. doi: 10.1080/07853890.2024.2397087. Epub 2024 Sep 6. Ann Med. 2024. PMID: 39239861 Free PMC article.
-
Guidelines for Antibiotics Prescription in Critically Ill Patients.Indian J Crit Care Med. 2024 Aug;28(Suppl 2):S104-S216. doi: 10.5005/jp-journals-10071-24677. Epub 2024 Aug 10. Indian J Crit Care Med. 2024. PMID: 39234229 Free PMC article.
-
Inhaled pH-Responsive polymyxin B-loaded albumin nanoparticles against pneumonia caused by carbapenem resistant Klebsiella pneumoniae.Mater Today Bio. 2025 Feb 18;31:101590. doi: 10.1016/j.mtbio.2025.101590. eCollection 2025 Apr. Mater Today Bio. 2025. PMID: 40104651 Free PMC article.
-
Clinical outcomes and pharmacokinetics/pharmacodynamics of intravenous polymyxin B treatment for various site carbapenem-resistant gram-negative bacterial infections: a prospective observational multicenter study.Antimicrob Agents Chemother. 2025 Apr 2;69(4):e0185924. doi: 10.1128/aac.01859-24. Epub 2025 Mar 6. Antimicrob Agents Chemother. 2025. PMID: 40047414 Free PMC article.
-
Efficacy and safety of different polymyxin-containing regimens for the treatment of pneumonia caused by multidrug-resistant gram-negative bacteria: a systematic review and network meta-analysis.Crit Care. 2024 Jul 14;28(1):239. doi: 10.1186/s13054-024-05031-w. Crit Care. 2024. PMID: 39004760 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
