

Using Alzheimer's disease blood tests to accelerate clinical trial enrollment
- PMID: 35934777
- PMCID: PMC9902574
- DOI: 10.1002/alz.12754
Using Alzheimer's disease blood tests to accelerate clinical trial enrollment
Abstract
Introduction: Screening potential participants in Alzheimer's disease (AD) clinical trials with amyloid positron emission tomography (PET) is often time consuming and expensive.
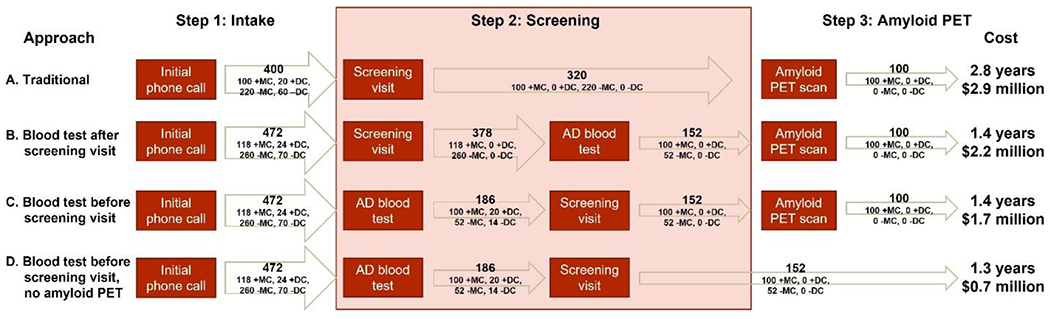
Methods: A web-based application was developed to model the time and financial cost of screening for AD clinical trials. Four screening approaches were compared; three approaches included an AD blood test at different stages of the screening process.
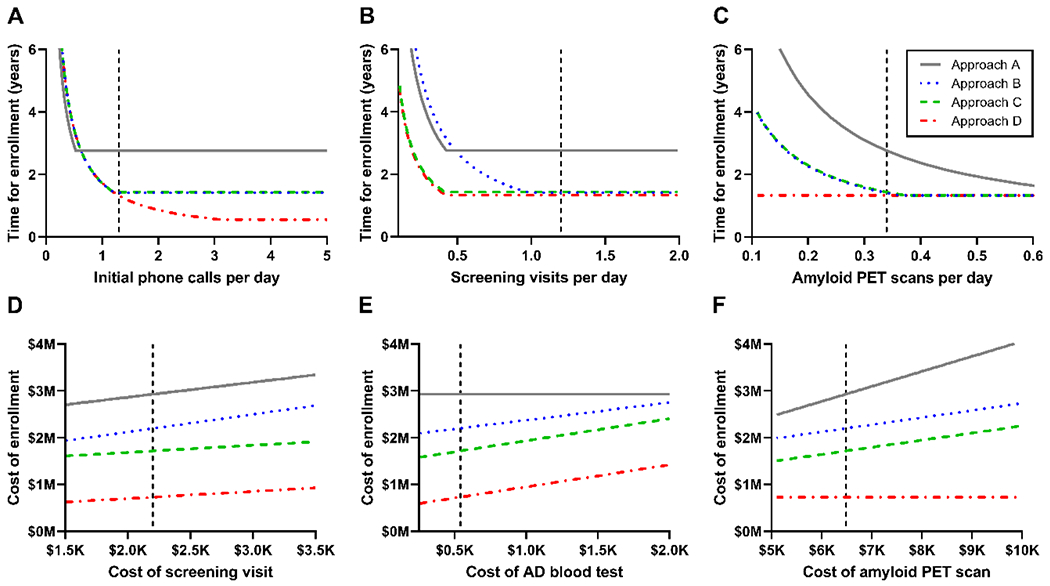
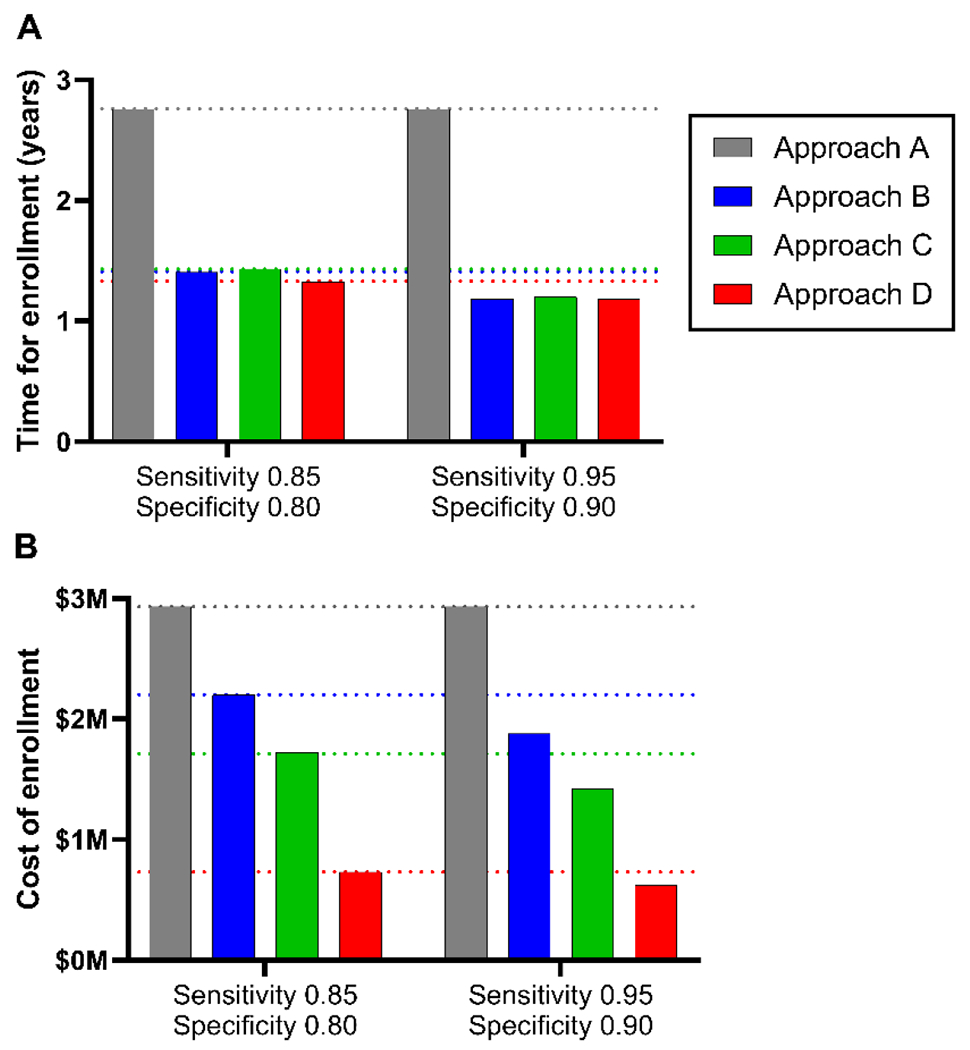
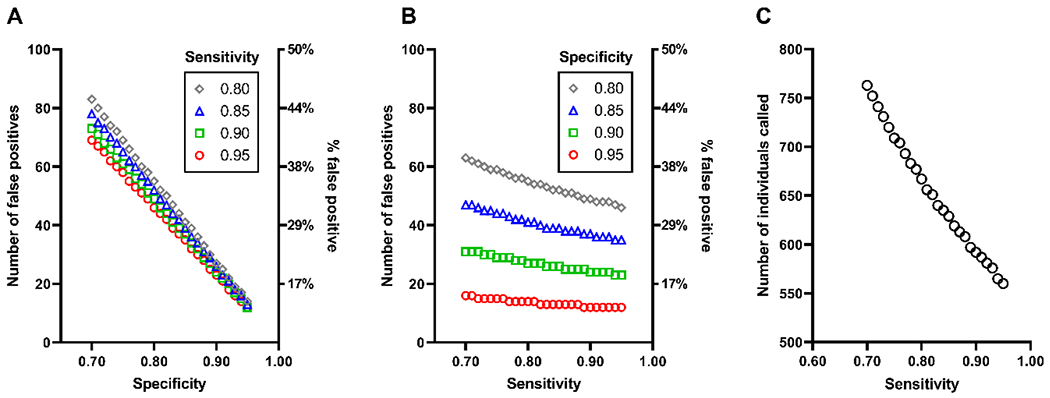
Results: The traditional screening approach using only amyloid PET was the most time consuming and expensive. Incorporating an AD blood test at any point in the screening process decreased both the time and financial cost of trial enrollment. Improvements in AD blood test accuracy over currently available tests only marginally increased savings. Use of a high specificity cut-off may improve the feasibility of screening with only an AD blood test.
Discussion: Incorporating AD blood tests into screening for AD clinical trials may reduce the time and financial cost of enrollment.
Highlights: The time and cost of enrolling participants in Alzheimer's disease (AD) clinical trials were modeled. A web-based application was developed to enable evaluation of key parameters. AD blood tests may decrease the time and financial cost of clinical trial enrollment. Improvements in AD blood test accuracy only marginally increased savings. Use of a high specificity cut-off may enable screening with only an AD blood test.
Keywords: Shiny app; amyloid positron emission tomography; blood tests; blood-based biomarkers; clinical trials; cost; economics; false negative; false positive; modeling; screening; screening approaches; time of enrollment.
© 2022 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
SES has analyzed data provided by C2N Diagnostics to Washington University, but she has not received any research funding or personal compensation from C2N Diagnostics or any other for-profit organizations. C2N Diagnostics had no role in this study, interpretation, or manuscript. YL, ML, AD, EP, LV, BHH, KW, BS, and MG report no disclosures. RJB and DMH co-founded C2N Diagnostics, which offers the PrecivityAD™ blood test. Washington University, RJB, and DMH have equity ownership interest in C2N Diagnostics and receive royalty income based on technology (stable isotope labeling kinetics and blood plasma assay) licensed by Washington University to C2N Diagnostics. RJB and DMH receive income from C2N Diagnostics for serving on the scientific advisory board. RJB has received honoraria as a speaker, consultant, or advisory board member from Amgen and Roche. DMH is on the scientific advisory board of Denali, Genentech, and Cajal Neuroscience and consults for Alector. Neither Dr. Morris nor his family owns stock or has equity interest (outside of mutual funds or other externally directed accounts) in any pharmaceutical or biotechnology company.
Figures

References
-
- Winblad B, Amouyel P, Andrieu S, Ballard C, Brayne C, Brodaty H, et al. Defeating Alzheimer’s disease and other dementias: a priority for European science and society. The Lancet Neurology. 2016;15:455–532. - PubMed
-
- Johnson KA, Minoshima S, Bohnen NI, Donohoe KJ, Foster NL, Herscovitch P, et al. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimer’s & dementia : the journal of the Alzheimer’s Association. 2013;9:e-1-16. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
