

Sex disparities in the incidence of 21 cancer types: Quantification of the contribution of risk factors
- PMID: 35934938
- PMCID: PMC11578066
- DOI: 10.1002/cncr.34390
Sex disparities in the incidence of 21 cancer types: Quantification of the contribution of risk factors
Abstract
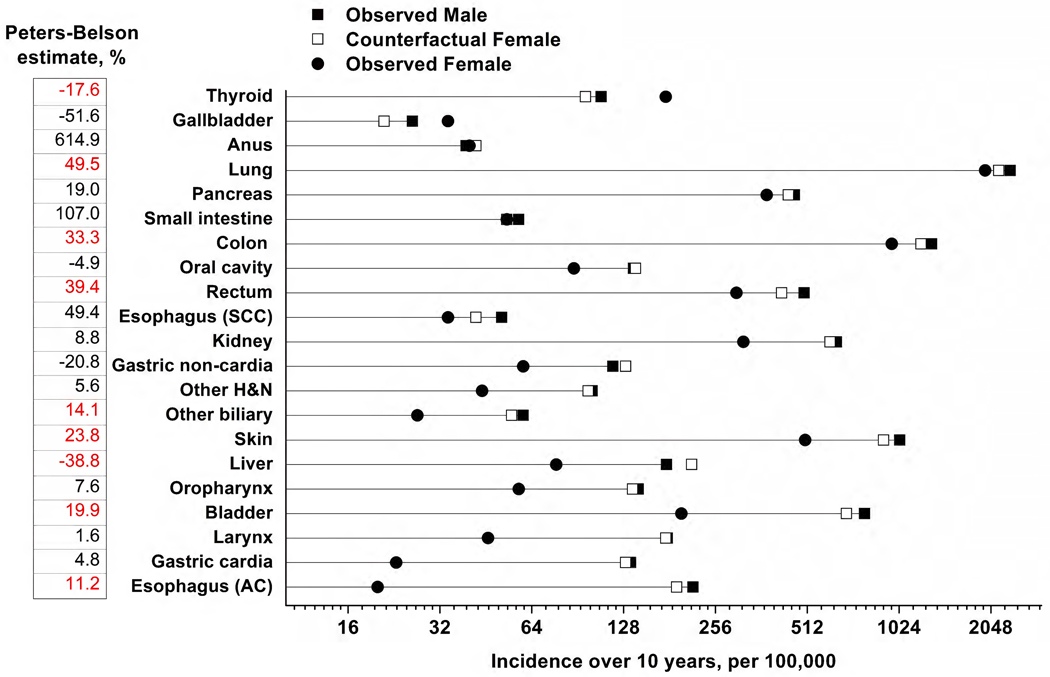
Background: Cancer incidence is higher in men than in women at most shared anatomic sites for currently unknown reasons. The authors quantified the extent to which behaviors (smoking and alcohol use), anthropometrics (body mass index and height), lifestyles (physical activity, diet, medications), and medical history collectively explain the male predominance of risk at 21 shared cancer sites.
Methods: Prospective cohort analyses (n = 171,274 male and n = 122,826 female participants; age range, 50-71 years) in the National Institutes of Health-AARP Diet and Health Study (1995-2011). Cancer-specific Cox regression models were used to estimate male-to-female hazard ratios (HRs). The degree to which risk factors explained the observed male-female risk disparity was quantified using the Peters-Belson method.
Results: There were 26,693 incident cancers (17,951 in men and 8742 in women). Incidence was significantly lower in men than in women only for thyroid and gallbladder cancers. At most other anatomic sites, the risks were higher in men than in women (adjusted HR range, 1.3-10.8), with the strongest increases for bladder cancer (HR, 3.33; 95% confidence interval [CI], 2.93-3.79), gastric cardia cancer (HR, 3.49; 95% CI, 2.26-5.37), larynx cancer (HR, 3.53; 95% CI, 2.46-5.06), and esophageal adenocarcinoma (HR, 10.80; 95% CI, 7.33-15.90). Risk factors explained a statistically significant (nonzero) proportion of the observed male excess for esophageal adenocarcinoma and cancers of liver, other biliary tract, bladder, skin, colon, rectum, and lung. However, only a modest proportion of the male excess was explained by risk factors (ranging from 50% for lung cancer to 11% for esophageal adenocarcinoma).
Conclusions: Men have a higher risk of cancer than women at most shared anatomic sites. Such male predominance is largely unexplained by risk factors, underscoring a role for sex-related biologic factors.
Keywords: cancer; health disparities; incidence; sex differences.
© 2022 American Cancer Society. This article has been contributed to by U.S. Government employees and their work is in the public domain in the USA.
Conflict of interest statement
Conflict of interest statement
None declared.
Figures
Comment in
-
Sex disparities in cancer: An ongoing quest.Cancer. 2022 Oct 1;128(19):3446-3448. doi: 10.1002/cncr.34389. Epub 2022 Aug 8. Cancer. 2022. PMID: 35934955 Free PMC article. No abstract available.
-
Reply to "Age-specific versus age-adjusted rates for the evaluation of the impact of the sex on cancer morbidity".Cancer. 2023 Feb 1;129(3):484. doi: 10.1002/cncr.34568. Epub 2022 Nov 25. Cancer. 2023. PMID: 36426985 No abstract available.
-
Age-specific versus age-adjusted rates for the evaluation of the impact of the sex on cancer morbidity.Cancer. 2023 Feb 1;129(3):483. doi: 10.1002/cncr.34569. Epub 2022 Nov 25. Cancer. 2023. PMID: 36426986 No abstract available.
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
