

Four-dimensional flow cardiac magnetic resonance assessment of left ventricular diastolic function
- PMID: 35935619
- PMCID: PMC9355735
- DOI: 10.3389/fcvm.2022.866131
Four-dimensional flow cardiac magnetic resonance assessment of left ventricular diastolic function
Abstract
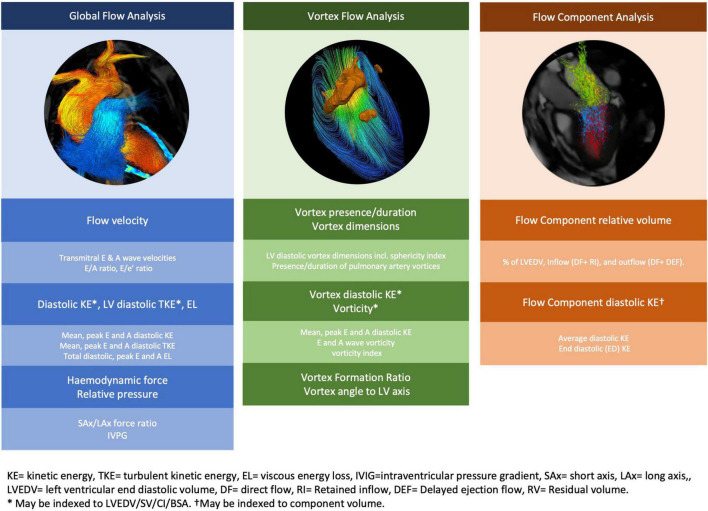
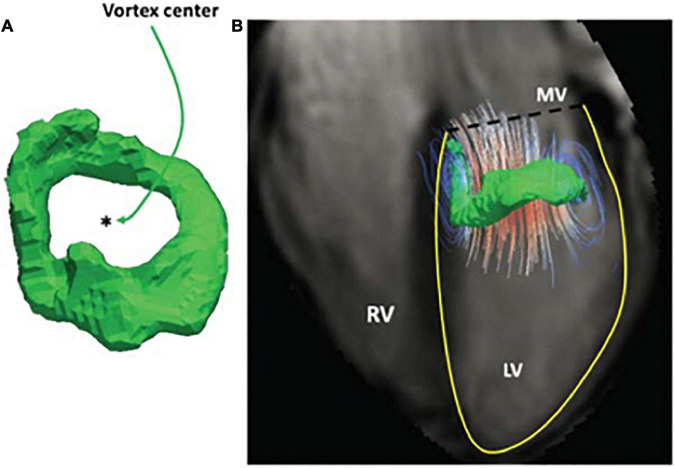
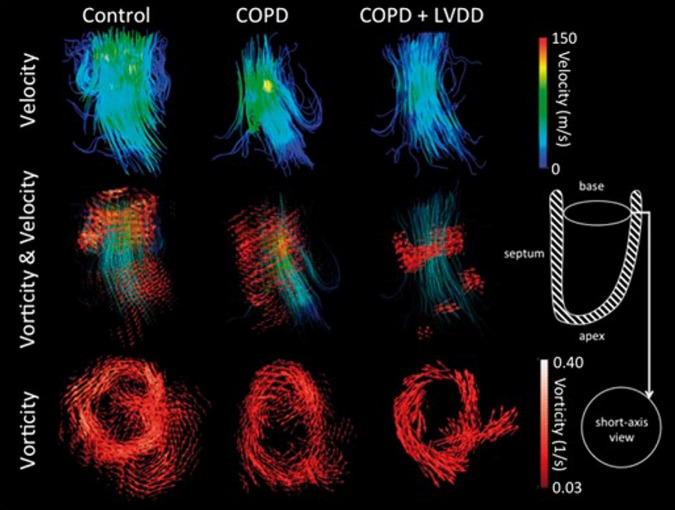
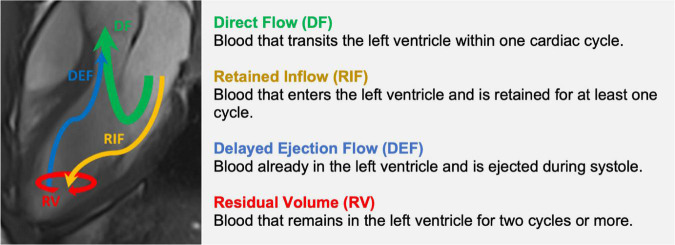
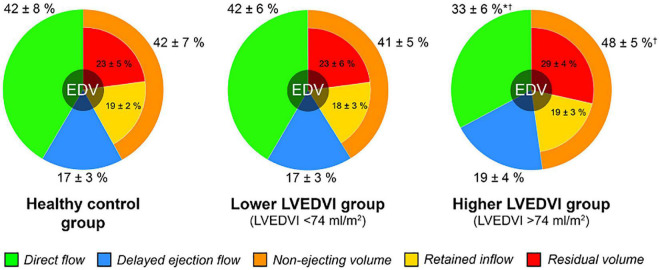
Left ventricular diastolic dysfunction is a major cause of heart failure and carries a poor prognosis. Assessment of left ventricular diastolic function however remains challenging for both echocardiography and conventional phase contrast cardiac magnetic resonance. Amongst other limitations, both are restricted to measuring velocity in a single direction or plane, thereby compromising their ability to capture complex diastolic hemodynamics in health and disease. Time-resolved three-dimensional phase contrast cardiac magnetic resonance imaging with three-directional velocity encoding known as '4D flow CMR' is an emerging technology which allows retrospective measurement of velocity and by extension flow at any point in the acquired 3D data volume. With 4D flow CMR, complex aspects of blood flow and ventricular function can be studied throughout the cardiac cycle. 4D flow CMR can facilitate the visualization of functional blood flow components and flow vortices as well as the quantification of novel hemodynamic and functional parameters such as kinetic energy, relative pressure, energy loss and vorticity. In this review, we examine key concepts and novel markers of diastolic function obtained by flow pattern analysis using 4D flow CMR. We consolidate the existing evidence base to highlight the strengths and limitations of 4D flow CMR techniques in the surveillance and diagnosis of left ventricular diastolic dysfunction.
Keywords: 4D flow cardiac MR; diastolic function; flow components; heart failure; kinetic energy; vortex.
Copyright © 2022 Ashkir, Myerson, Neubauer, Carlhäll, Ebbers and Raman.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Tribouilloy C, Rusinaru D, Mahjoub H, Soulière V, Lévy F, Peltier M, et al. Prognosis of heart failure with preserved ejection fraction: a 5 year prospective population-based study. Eur Heart J. (2008) 29:339–47. - PubMed
-
- Garg A, Hummel SL. Diastolic heart failure. Inpatient Cardiovasc Med. (2013) 45:166–77.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources