

Comparative analysis of left atrial appendage closure efficacy and outcomes by CHA2DS2-VASc score group in patients with non-valvular atrial fibrillation
- PMID: 35935622
- PMCID: PMC9353551
- DOI: 10.3389/fcvm.2022.905728
Comparative analysis of left atrial appendage closure efficacy and outcomes by CHA2DS2-VASc score group in patients with non-valvular atrial fibrillation
Abstract
Background: Higher CHA2DS2-VASc score is associated with an increased risk of adverse cardio-cerebrovascular events in patients with non-valvular atrial fibrillation (NVAF), regardless of oral anticoagulation (OAC) status. However, whether this association still exists in patients undergoing left atrial appendage closure (LAAC) is unknown. We evaluated the impact of CHA2DS2-VASc score on LAAC efficacy and outcomes.
Methods: A total of 401 consecutive patients undergoing LAAC were included and divided into 3 groups based on CHA2DS2-VASc score (0-2, 3-4, and ≥5). Baseline characteristics, periprocedural complications, and long-term outcomes were collected and compared across all groups.
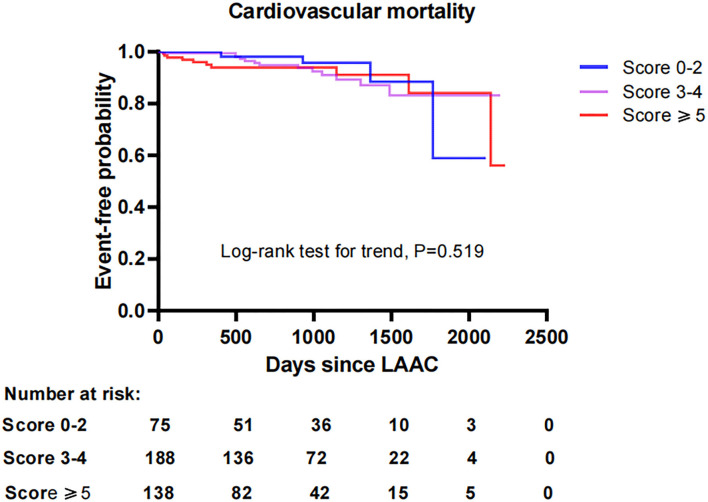
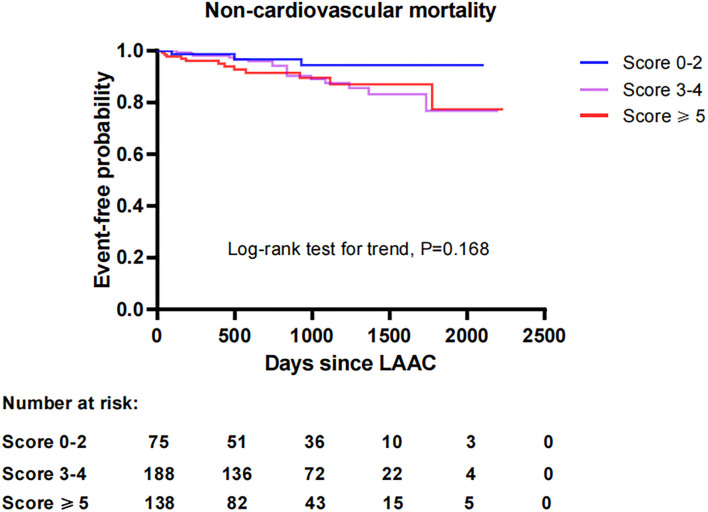
Results: There were no significant differences in implantation success, periprocedural complications, and long-term outcomes across all score groups. Kaplan-Meier estimation showed that the cumulative ratio of freedom from all-cause mortality (P = 0.146), cardiovascular mortality (P = 0.519), and non-cardiovascular mortality (P = 0.168) did not differ significantly by CHA2DS2-VASc score group. LAAC decreased the risks of thromboembolism and major bleeding, resulting in a relative risk reduction (RRR) of 82.4% (P < 0.001) and 66.7% (P < 0.001) compared with expected risks in the overall cohort, respectively. Subgroup analysis indicated that observed risks of thromboembolism and major bleeding were significantly lower than the expected risks in score 3-4 and score ≥5 groups, respectively. The level of RRR increased with CHA2DS2-VASc score (P < 0.001 for trend) for thromboembolism but not for major bleeding (P = 0.2729 for trend).
Conclusion: Patients with higher CHA2DS2-VASc score did not experience worse outcomes, which may be partly attributed to more benefits provided by LAAC intervention in such patients compared to those with a low score.
Keywords: CHA2DS2-VASc score; atrial fibrillation; left atrial appendage closure; major bleeding; outcomes; stroke.
Copyright © 2022 Zhao, Zhao, Hou, Post, Herold, Walsleben, Yuan, Meng and Yu.
Figures



Similar articles
-
Left Atrial Appendage Closure Yields Favorable Cardio- and Cerebrovascular Outcomes in Patients With Non-valvular Atrial Fibrillation and Prior Stroke.Front Neurol. 2022 Jan 10;12:784557. doi: 10.3389/fneur.2021.784557. eCollection 2021. Front Neurol. 2022. PMID: 35082747 Free PMC article.
-
Left Atrial Appendage Closure Versus Direct Oral Anticoagulants in High-Risk Patients With Atrial Fibrillation.J Am Coll Cardiol. 2020 Jun 30;75(25):3122-3135. doi: 10.1016/j.jacc.2020.04.067. J Am Coll Cardiol. 2020. PMID: 32586585 Clinical Trial.
-
Efficacy and safety of left atrial appendage closure in non-valvular atrial fibrillation in patients over 75 years.Heart Vessels. 2019 Nov;34(11):1858-1865. doi: 10.1007/s00380-019-01428-8. Epub 2019 May 29. Heart Vessels. 2019. PMID: 31144099
-
Systematic review on left atrial appendage closure with the LAmbre device in patients with non-valvular atrial fibrillation.BMC Cardiovasc Disord. 2020 Feb 12;20(1):78. doi: 10.1186/s12872-020-01349-9. BMC Cardiovasc Disord. 2020. PMID: 32050904 Free PMC article.
-
Left Atrial Appendage Closure Versus Oral Anticoagulation in Non-Valvular Atrial Fibrillation: A Systematic Review and Meta-Analysis.Cardiovasc Revasc Med. 2022 Mar;36:18-24. doi: 10.1016/j.carrev.2021.04.019. Epub 2021 Apr 22. Cardiovasc Revasc Med. 2022. PMID: 33903038
References
-
- Ruff CT, Giugliano RP, Braunwald E, Hoffman EB, Deenadayalu N, Ezekowitz MD, et al. . Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. (2014) 383:955–62. 10.1016/S0140-6736(13)62343-0 - DOI - PubMed
LinkOut - more resources
Full Text Sources