

Association between baseline smoking status and clinical outcomes following myocardial infarction
- PMID: 35935630
- PMCID: PMC9354586
- DOI: 10.3389/fcvm.2022.918033
Association between baseline smoking status and clinical outcomes following myocardial infarction
Abstract
Background: Whether the effect of smoking on clinical outcomes following an acute myocardial infarction (AMI) is beneficial or detrimental remains inconclusive. We invesetigated the effect of smoking on the clinical outcomes in patients following an AMI.
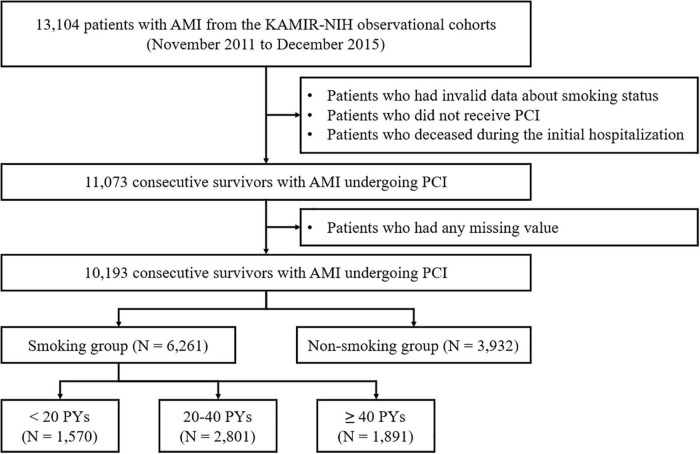
Methods: Among 13,104 patients between November 2011 and June 2015 from a nationwide Korean AMI registry, a total of 10,193 participants were extracted then classified into two groups according to their smoking habit: (1) smoking group (n = 6,261) and (2) non-smoking group (n = 3,932). The participants who smoked were further subclassified according to their smoking intensity quantified by pack years (PYs): (1) <20 PYs (n = 1,695); (2) 20-40 PYs (n = 3,018); and (3) ≥40 PYs (n = 2,048). Each group was compared to each other according to treatment outcomes. The primary outcome was the incidence of major adverse cardiac and cerebrovascular events (MACCEs), which is a composite of all-cause mortality, non-fatal MI (NFMI), any revascularization, cerebrovascular accident, rehospitalization, and stent thrombosis. Secondary outcomes included the individual components of MACCEs. The Cox proportional hazard regression method was used to evaluate associations between baseline smoking and clinical outcomes following an AMI. Two propensity score weighting methods were performed to adjust for confounders, including propensity score matching and inverse probability of treatment weighting.
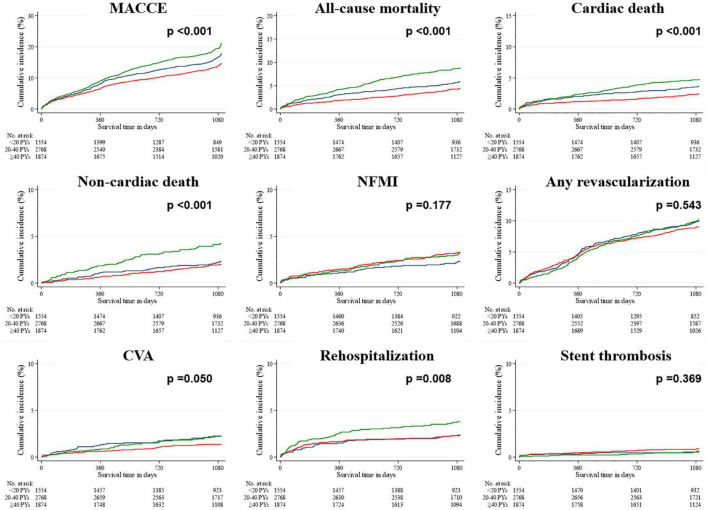
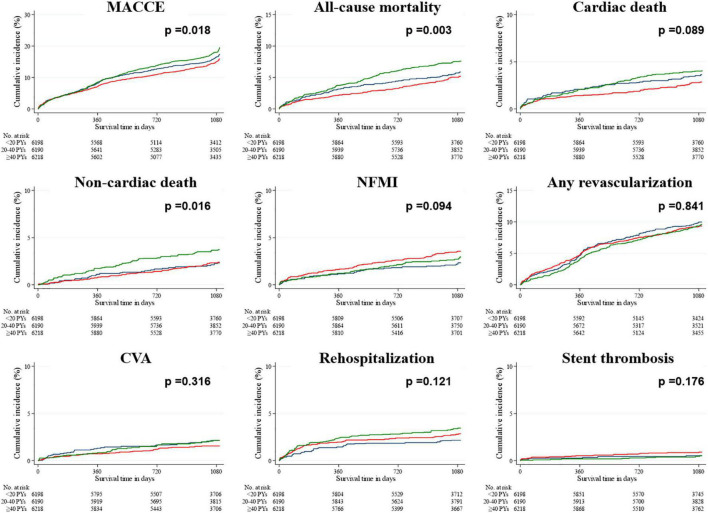
Results: While the incidence of all clinical outcomes, except for stent thrombosis, was lower in the smoking group than in the non-smoking group in the unadjusted data, the covariates-adjusted data showed statistical attenuation of these differences but a higher all-cause mortality in the smoking group. For smokers, the incidence of MACCEs, all-cause mortality, cardiac and non-cardiac death, and rehospitalization was significantly different between the groups, with the highest rates of MACCE, all-cause mortality, non-cardiac death, and rehospitalization in the group with the highest smoking intensity. These differences were statistically attenuated in the covariates-adjusted data, except for MACCEs, all-cause mortality, and non-cardiac death, which had the highest incidence in the group with ≥40 PYs.
Conclusion: Smoking had no beneficial effect on the clinical outcomes following an AMI. Moreover, for those who smoked, clinical outcomes tended to deteriorate as smoking intensity increased.
Keywords: coronary artery disease; ischemic heart disease; myocardial infarction; smoking; treatment outcome.
Copyright © 2022 Oh, Kim, Cho, Kim, Sim, Hong, Ahn and Jeong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Comparison on the long-term outcomes post percutaneous coronary intervention or coronary artery bypass grafting for bifurcation lesions in unprotected left main coronary artery].Zhonghua Xin Xue Guan Bing Za Zhi. 2017 Jan 25;45(1):19-25. doi: 10.3760/cma.j.issn.0253-3758.2017.01.005. Zhonghua Xin Xue Guan Bing Za Zhi. 2017. PMID: 28100341 Chinese.
-
[Efficacy comparison of primary percutaneous coronary intervention by drug-coated balloon angioplasty or drug-eluting stenting in acute myocardial infarction patients with de novo coronary lesions].Zhonghua Xin Xue Guan Bing Za Zhi. 2020 Jul 24;48(7):600-607. doi: 10.3760/cma.j.cn112148-20200327-00254. Zhonghua Xin Xue Guan Bing Za Zhi. 2020. PMID: 32842271 Chinese.
-
Impact of P2Y12 inhibitors on cardiovascular outcomes of Korean acute myocardial infarction patients with baseline thrombocytopenia.Front Cardiovasc Med. 2022 Sep 14;9:921955. doi: 10.3389/fcvm.2022.921955. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36186989 Free PMC article.
-
[Outcome of patients with coronary artery disease and left ventricular ejection fraction less than 50% undergoing percutaneous coronary intervention].Zhonghua Xin Xue Guan Bing Za Zhi. 2017 Dec 24;45(12):1058-1066. doi: 10.3760/cma.j.issn.0253-3758.2017.12.010. Zhonghua Xin Xue Guan Bing Za Zhi. 2017. PMID: 29325366 Chinese.
-
Beta-blockers for suspected or diagnosed acute myocardial infarction.Cochrane Database Syst Rev. 2019 Dec 17;12(12):CD012484. doi: 10.1002/14651858.CD012484.pub2. Cochrane Database Syst Rev. 2019. PMID: 31845756 Free PMC article.
Cited by
-
Patient-Related Factors Predicting Stent Thrombosis in Percutaneous Coronary Interventions.J Clin Med. 2023 Nov 28;12(23):7367. doi: 10.3390/jcm12237367. J Clin Med. 2023. PMID: 38068419 Free PMC article. Review.
-
The Effects of Nicotine on Re-endothelialization, Inflammation, and Neoatherosclerosis After Drug-Eluting Stent Implantation in a Porcine Model.Korean Circ J. 2025 Jan;55(1):50-64. doi: 10.4070/kcj.2024.0171. Epub 2024 Sep 30. Korean Circ J. 2025. PMID: 39434360 Free PMC article.
-
Smoking, immunity, and cardiovascular prognosis: a study of plasma IgE concentration in patients with acute myocardial infarction.Front Cardiovasc Med. 2023 Sep 5;10:1174081. doi: 10.3389/fcvm.2023.1174081. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37731521 Free PMC article.
-
Unfolding the reality of the smoking paradox in a South Asian cohort of patients presenting with ST-elevation acute coronary syndrome undergoing primary percutaneous coronary intervention.SAGE Open Med. 2023 Oct 27;11:20503121231206932. doi: 10.1177/20503121231206932. eCollection 2023. SAGE Open Med. 2023. PMID: 37900968 Free PMC article.
-
Smoking behaviour in post-acute myocardial infarction patients: cross-sectional study.Ann Med Surg (Lond). 2024 Apr 3;86(5):2531-2537. doi: 10.1097/MS9.0000000000001333. eCollection 2024 May. Ann Med Surg (Lond). 2024. PMID: 38694391 Free PMC article.
References
-
- Zou Z, Cini K, Dong B, Ma Y, Ma J, Burgner DP, et al. Time trends in cardiovascular disease mortality across the BRICS: an age-period-cohort analysis of key nations with emerging economies using the global burden of disease Study 2017. Circulation. (2020) 141:790–9. 10.1161/CIRCULATIONAHA.119.042864 - DOI - PubMed
-
- Dagenais GR, Leong DP, Rangarajan S, Lanas F, Lopez-Jaramillo P, Gupta R, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. (2020) 395:785–94. 10.1016/S0140-6736(19)32007-0 - DOI - PubMed
-
- Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P, et al. Acute myocardial infarction: changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI program (French registry of acute ST-elevation or non-ST-elevation myocardial infarction) 1995 to 2015. Circulation. (2017) 136:1908–19. - PubMed
LinkOut - more resources
Full Text Sources