

Predictors of late arrhythmic events after generator replacement in Brugada syndrome treated with prophylactic ICD
- PMID: 35935654
- PMCID: PMC9355272
- DOI: 10.3389/fcvm.2022.964694
Predictors of late arrhythmic events after generator replacement in Brugada syndrome treated with prophylactic ICD
Erratum in
-
Corrigendum: Predictors of late arrhythmic events after generator replacement in Brugada syndrome treated with prophylactic ICD.Front Cardiovasc Med. 2022 Nov 15;9:1076294. doi: 10.3389/fcvm.2022.1076294. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36457801 Free PMC article.
Abstract
Introduction: Predictors of late life-threatening arrhythmic events in Brugada syndrome (BrS) patients who received a prophylactic ICD implantation remain to be evaluated. The aim of the present long-term multicenter study was to assess the incidence and clinical-electrocardiographic predictors of late life-threatening arrhythmic events in BrS patients with a prophylactic implantable cardioverter defibrillator (ICD) and undergoing generator replacement (GR).
Methods: The study population included 105 patients (75% males; mean age 45 ± 14years) who received a prophylactic ICD and had no arrhythmic event up to first GR.
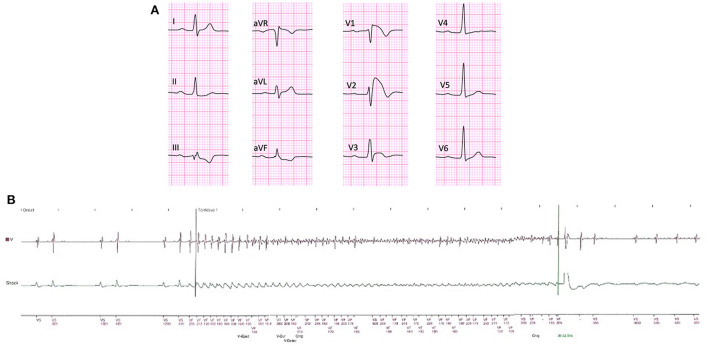
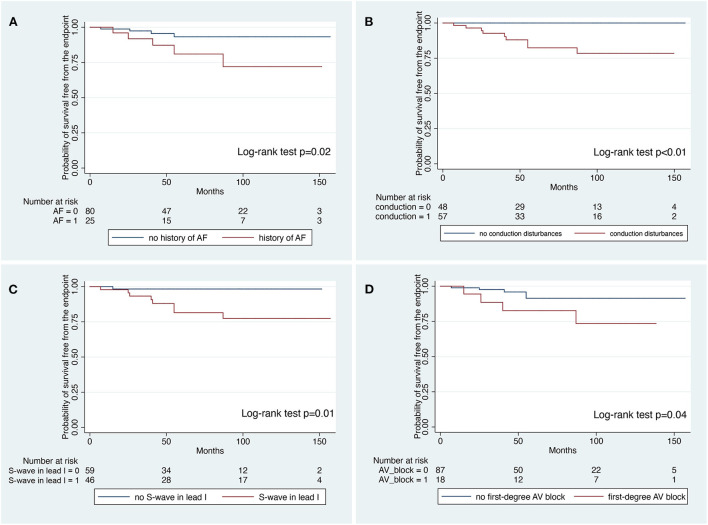
Results: The median period from first ICD implantation to last follow-up was 155 (128-181) months and from first ICD Implantation to the GR was 84 (61-102) months. During a median follow-up of 57 (38-102) months after GR, 10 patients (9%) received successful appropriate ICD intervention (1.6%/year). ICD interventions included shock on ventricular fibrillation (n = 8 patients), shock on ventricular tachycardia (n = 1 patient), and antitachycardia pacing on ventricular tachycardia (n = 1 patient). At survival analysis, history of atrial fibrillation (log-rank test; P = 0.02), conduction disturbances (log-rank test; P < 0.01), S wave in lead I (log-rank test; P = 0.01) and first-degree atrioventricular block (log-rank test; P = 0.04) were significantly associated with the occurrence of late appropriate ICD intervention. At Cox-regression multivariate analysis, S-wave in lead I was the only independent predictor of late appropriate ICD intervention (HR: 9.17; 95%CI: 1.15-73.07; P = 0.03).
Conclusions: The present study indicates that BrS patient receiving a prophylactic ICD may experience late appropriate intervention after GR in a clinically relevant proportion of cases. S-wave in lead I at the time of first clinical evaluation was the only independent predictor of persistent risk of life-threatening arrhythmic events. These findings support the need for GR at the end of service regardless of previous appropriate intervention, mostly in BrS patients with conduction abnormalities.
Keywords: Brugada syndrome; complications; implantable cardioverter-defibrillator; risk stratification; sudden cardiac death.
Copyright © 2022 Migliore, Martini, Calo', Martino, Winnicki, Vio, Condello, Rizzo, Zorzi, Pannone, Miraglia, Sieira, Chierchia, Curcio, Allocca, Mantovan, Salghetti, Curnis, Bertaglia, De Lazzari, de Asmundis and Corrado.
Conflict of interest statement
VM received an educational grant from the Enrico and Enrica Sovena Fundation, Italy. G-BC received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Boston Scientific, Acutus Medical. CA receives research grants on behalf of the center from Biotronik, Medtronic, Abbott, LivaNova, Boston Scientific, AtriCure, Philips, Acutus, and received compensation for teaching purposes and proctoring from Medtronic, Abbott, Biotronik, Livanova, Boston Scientific, Atricure, Acutus Medical, and Daiichi Sankyo. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Factors predisposing to ventricular tachyarrhythmia leading to appropriate ICD intervention in patients with coronary artery disease or non-ischaemic dilated cardiomyopathy.Kardiol Pol. 2012;70(12):1264-75. Kardiol Pol. 2012. PMID: 23264245
-
Time-to-first appropriate shock in patients implanted prophylactically with an implantable cardioverter-defibrillator: data from the Survey on Arrhythmic Events in BRUgada Syndrome (SABRUS).Europace. 2019 May 1;21(5):796-802. doi: 10.1093/europace/euy301. Europace. 2019. PMID: 30590530
-
Incidence of Ventricular Arrhythmias and 1-Year Predictors of Mortality in Patients Treated With Implantable Cardioverter-Defibrillator Undergoing Generator Replacement.J Am Heart Assoc. 2021 Feb 16;10(4):e018090. doi: 10.1161/JAHA.120.018090. Epub 2021 Jan 30. J Am Heart Assoc. 2021. PMID: 33522246 Free PMC article.
-
Incidence of appropriate anti-tachycardia therapies after elective generator replacement in patient with heart failure initially implanted with a defibrillator for primary prevention: Results of a meta-analysis.Int J Cardiol. 2019 May 15;283:122-127. doi: 10.1016/j.ijcard.2018.12.068. Epub 2019 Jan 2. Int J Cardiol. 2019. PMID: 30638746 Review.
-
Systematic review for the 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society.Heart Rhythm. 2018 Oct;15(10):e253-e274. doi: 10.1016/j.hrthm.2017.10.037. Epub 2017 Nov 4. Heart Rhythm. 2018. PMID: 29097318
Cited by
-
Appropriate and inappropriate therapies in patients with Brugada syndrome. What to expect? Authors' reply.Europace. 2023 Aug 2;25(9):euad251. doi: 10.1093/europace/euad251. Europace. 2023. PMID: 37611198 Free PMC article. No abstract available.
-
Beyond the type 1 pattern: comprehensive risk stratification in Brugada syndrome.J Interv Card Electrophysiol. 2025 Aug 6. doi: 10.1007/s10840-025-02101-z. Online ahead of print. J Interv Card Electrophysiol. 2025. PMID: 40767905 Review.
-
Marked PR interval variability in a patient with Brugada syndrome.Porto Biomed J. 2023 Apr 10;8(2):e209. doi: 10.1097/j.pbj.0000000000000209. eCollection 2023 Mar-Apr. Porto Biomed J. 2023. PMID: 37152631 Free PMC article. No abstract available.
-
Ventricular fibrillation induced by fever in structurally normal hearts.Front Cardiovasc Med. 2023 Sep 25;10:1230295. doi: 10.3389/fcvm.2023.1230295. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37817866 Free PMC article. Review.
References
-
- Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, et al. . HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, EHRA, and APHRS in May 2013 and by ACCF. AHA, PACES, and AEPC in June 2013. Heart Rhythm. (2013) 10:1932–63. 10.1016/j.hrthm.2013.05.014 - DOI - PubMed
LinkOut - more resources
Full Text Sources