

Efficacy and Safety of Exploring Deeper Sections of the Infrapapillary Area of the Duodenum by Using Sedative Esophagogastroduodenoscopy
- PMID: 35935715
- PMCID: PMC9348967
- DOI: 10.1155/2022/1381299
Efficacy and Safety of Exploring Deeper Sections of the Infrapapillary Area of the Duodenum by Using Sedative Esophagogastroduodenoscopy
Abstract
Background: Using conventional esophagogastroduodenoscopy (EGD) to evaluate the infrapapillary area is not feasible. The use of sedative EGD may enable endoscopists to investigate the infrapapillary condition of the duodenum. In this study, we aimed to evaluate lesions in the infrapapillary regions by using sedative EGD.
Methods: In this retrospective observational study, we used the data of patients who underwent sedative EGD examinations at a tertiary hospital in southern Taiwan. The endoscopists evaluated the esophagus, stomach, and proximal duodenum and then attempted to explore the infrapapillary portion of the duodenum as deeply as possible. We assessed the success rate for the exploration of infrapapillary areas. Furthermore, we analyzed specific clinical findings of sedative EGD examination.
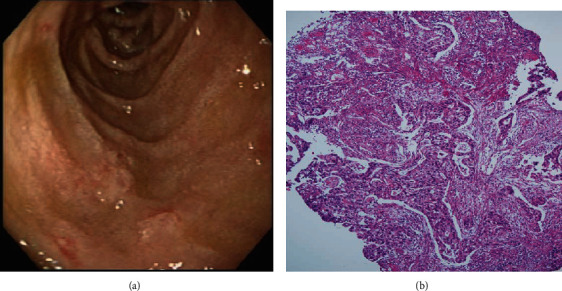
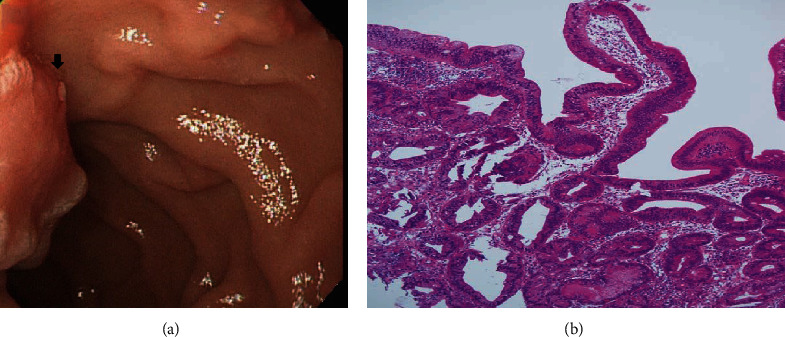
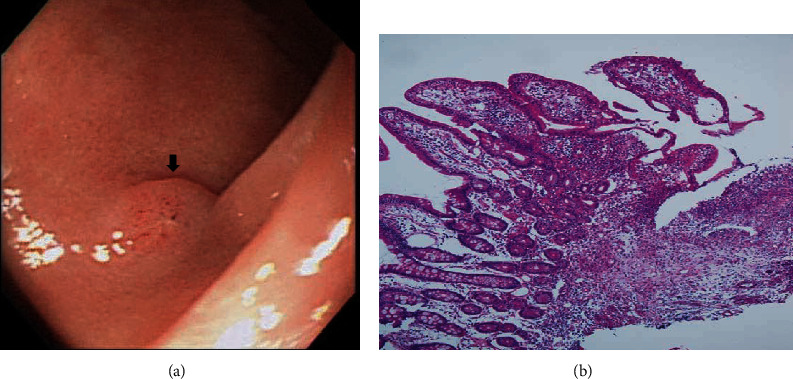
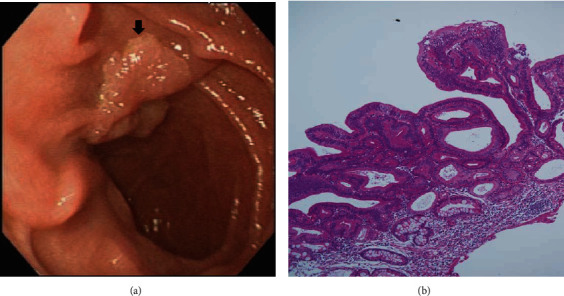
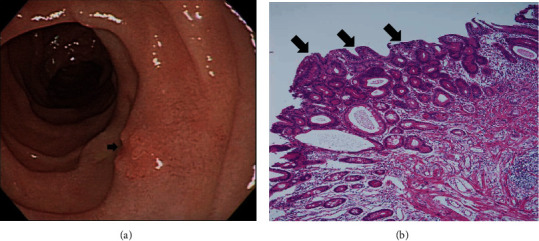
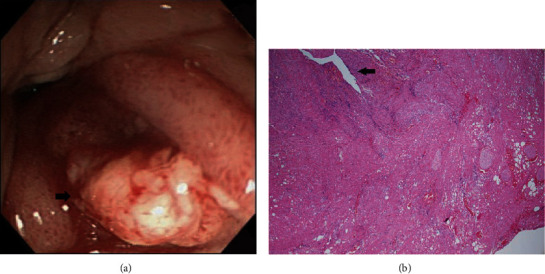
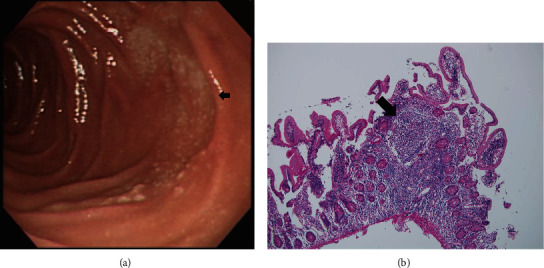
Results: In total, 2973 patients underwent sedative EGD between November 1, 2010, and December 31, 2011. For 2632 of these patients, it was their first sedative EGD examination. In 2511 patients (95.4%), the exploration of the infrapapillary areas was successful. In approximately 10% of the patients, specific findings were detected over the infrapapillary region, and 7 of these patients exhibited clinically significant findings (i.e., gallbladder cancer with metastasis, periampullary Vater adenoma, natural killer cell enteropathy, villous adenoma with moderate dysplasia, infrapapillary duodenal adenoma with dysplasia, duodenal perforation with tumor-like formation, and follicular lymphoma). No patient experienced minor or major adverse reactions during the sedative EGD procedure.
Conclusions: The current study provided evidence that sedative EGD examination enables a safe, comfortable, and effective endoscopic examination of deeper sections of the duodenum to evaluate the papillary and infrapapillary regions.
Copyright © 2022 Ming-Tse Hsu et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Role of esophagogastroduodenoscopy in detecting distal duodenal lesions: A single-center pilot study in Southern China.J Dig Dis. 2017 Nov;18(11):618-624. doi: 10.1111/1751-2980.12549. J Dig Dis. 2017. PMID: 29024444
-
A study of the safety and clinical efficacy of esophagogastroduodenoscopy after esophageal, gastric, or duodenal surgery in 60 patients.Am J Gastroenterol. 1995 Aug;90(8):1268-72. Am J Gastroenterol. 1995. PMID: 7639228
-
Longer Observation Time Increases Proportion of Neoplasms Detected by Esophagogastroduodenoscopy.Gastroenterology. 2017 Aug;153(2):460-469.e1. doi: 10.1053/j.gastro.2017.05.009. Epub 2017 May 10. Gastroenterology. 2017. PMID: 28501581
-
Comparison of procedural sequence in same-day bidirectional endoscopy: a systematic review and meta-analysis.Korean J Intern Med. 2020 Mar;35(2):331-341. doi: 10.3904/kjim.2019.319. Epub 2019 Dec 27. Korean J Intern Med. 2020. PMID: 31875664 Free PMC article.
-
Current status and evaluation of transnasal esophagogastroduodenoscopy.Dig Endosc. 2009 Jul;21(3):141-6. doi: 10.1111/j.1443-1661.2009.00891.x. Dig Endosc. 2009. PMID: 19691759 Review.
References
-
- Yoon Y. S., Kim S. W., Park S. J., et al. Clinicopathologic analysis of early ampullary cancers with a focus on the feasibility of ampullectomy. Annals of Surgery . 2005;242(1):92–100. doi: 10.1097/01.sla.0000167853.04171.bb. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
