

Local and Systemic Immunity Are Impaired in End-Stage-Renal-Disease Patients Treated With Hemodialysis, Peritoneal Dialysis and Kidney Transplant Recipients Immunized With BNT162b2 Pfizer-BioNTech SARS-CoV-2 Vaccine
- PMID: 35935974
- PMCID: PMC9354587
- DOI: 10.3389/fimmu.2022.832924
Local and Systemic Immunity Are Impaired in End-Stage-Renal-Disease Patients Treated With Hemodialysis, Peritoneal Dialysis and Kidney Transplant Recipients Immunized With BNT162b2 Pfizer-BioNTech SARS-CoV-2 Vaccine
Abstract
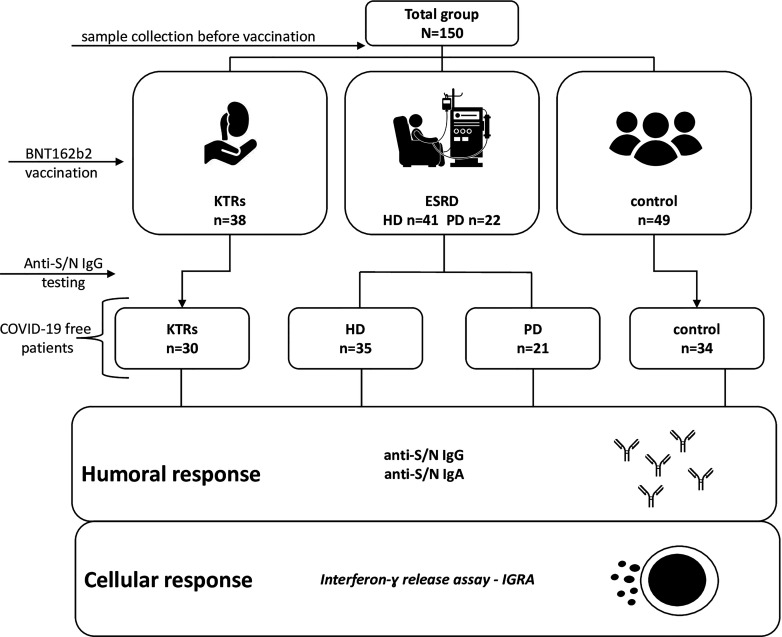
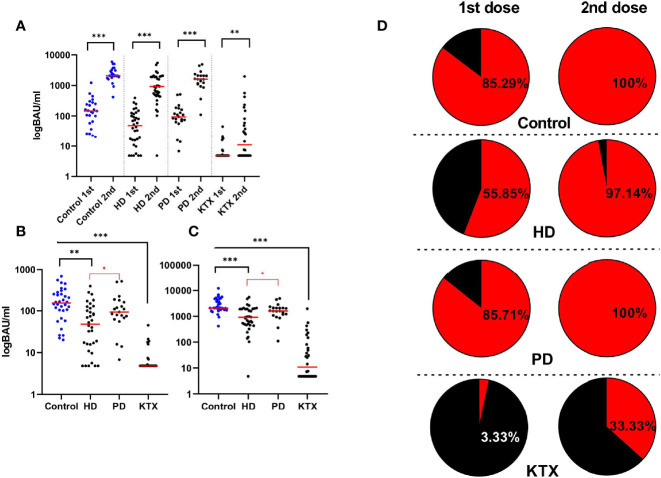
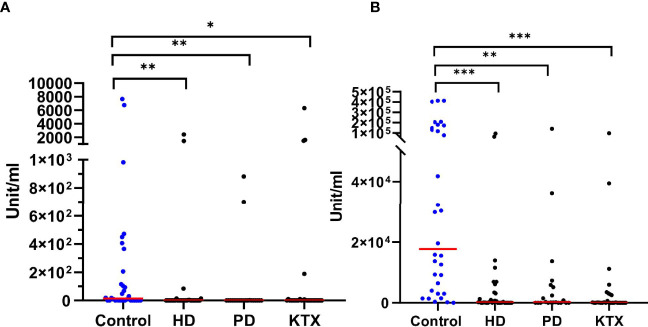
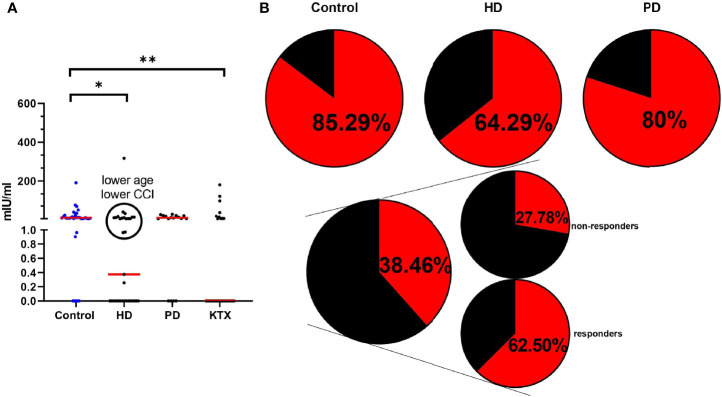
Vaccination against COVID-19 in patients with end-stage renal disease (ESRD) on replacement therapy and kidney transplant recipients (KTRs) is particularly important due to the high mortality rate. Here, we tested the local and systemic immunity to the novel Pfizer BioNTech (BNT162b2) messenger RNA (mRNA) in ESRD, KTR patients, and healthy individuals (150 subjects). The ESRD group was divided into: hemodialysis (HD) and peritoneal dialysis (PD). We investigated the local and systemic immunity based on anti-N (nucleoprotein) and anti-S (spike1/2) Immunoglobulin A (IgA) and Immunoglobulin G (IgG) antibodies, respectively. Additionally, we performed an Interferon gamma (IFN-γ) release test Interferon-gamma release assay (IGRA) to monitor the cellular component of vaccine response. The control group had the highest level of anti-S IgG antibodies (153/2,080 binding antibody units (BAU)/ml) among all analyzed patients after the 1st and 2nd dose, respectively. The HD group (48/926 BAU/ml) had a diminished antibody level compared to PD (93/1,607 BAU/ml). Moreover, the seroconversion rate after the 1st dose was lower in HD than PD (56% vs. 86%). KTRs had extremely low seroconversion (33%). IgA-mediated immunity was the most effective in the control group, while other patients had diminished IgA production. We observed a lower percentage of vaccine responders based on the IFN-γ level in all research participants (100% vs. 85% in control, 100% vs. 80% in PD, 97% vs. 64% in HD). 63% of seropositive KTRs had a positive IGRA, while 28% of seronegative patients produced IFN-γ. Collectively, PD patients had the strongest response among ESRD patients. Two doses of the Pfizer vaccine are ineffective, especially in HD and KTRs. A closer investigation of ESRD and KTRs is required to set the COVID-19 vaccine clinical guidance.
Clinical trial registration number: www.ClinicalTrials.gov, identifier: NCT04 905 862.
Trial registration: ClinicalTrials.gov NCT04905862.
Keywords: COVID-19; SARS-CoV-2; hemodialysis; peritoneal dialysis; transplantation.
Copyright © 2022 Piotrowska, Zieliński, Tylicki, Biedunkiewicz, Kubanek, Ślizień, Polewska, Tylicki, Muchlado, Sakowska, Renke, Sudoł, Dąbrowska, Lichodziejewska-Niemierko, Smiatacz, Dębska-Ślizień and Trzonkowski.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Humoral and cellular immune response to SARS-CoV-2 mRNA BNT162b2 vaccine in pediatric kidney transplant recipients compared with dialysis patients and healthy children.Pediatr Nephrol. 2023 Jul;38(7):2199-2208. doi: 10.1007/s00467-022-05813-w. Epub 2022 Dec 2. Pediatr Nephrol. 2023. PMID: 36459243 Free PMC article.
-
Impaired Immune Response to SARS-CoV-2 Vaccination in Dialysis Patients and in Kidney Transplant Recipients.Kidney360. 2021 Jul 13;2(9):1491-1498. doi: 10.34067/KID.0003512021. eCollection 2021 Sep 30. Kidney360. 2021. PMID: 35373105 Free PMC article.
-
The Safety and Immunogenicity of the mRNA-BNT162b2 SARS-CoV-2 Vaccine in Hemodialysis Patients.Front Immunol. 2021 Jun 16;12:704773. doi: 10.3389/fimmu.2021.704773. eCollection 2021. Front Immunol. 2021. PMID: 34220867 Free PMC article.
-
Humoral and cellular immune response to severe acute respiratory syndrome coronavirus-2 vaccination in haemodialysis and kidney transplant patients.Nephrology (Carlton). 2022 Jan;27(1):7-24. doi: 10.1111/nep.13974. Epub 2021 Sep 27. Nephrology (Carlton). 2022. PMID: 34510645 Free PMC article. Review.
-
A systematic review assessing the effectiveness of COVID-19 mRNA vaccines in chronic kidney disease (CKD) individuals.F1000Res. 2022 Aug 8;11:909. doi: 10.12688/f1000research.122820.2. eCollection 2022. F1000Res. 2022. PMID: 36531259 Free PMC article.
Cited by
-
Immune Status and SARS-CoV-2 Viral Dynamics.J Infect Dis. 2023 Aug 31;228(Suppl 2):S111-S116. doi: 10.1093/infdis/jiad200. J Infect Dis. 2023. PMID: 37650232 Free PMC article. Clinical Trial.
-
Predicting immunogenicity of COVID-19 vaccines in hemodialysis patients with renal disease.Heliyon. 2024 Mar 7;10(6):e27594. doi: 10.1016/j.heliyon.2024.e27594. eCollection 2024 Mar 30. Heliyon. 2024. PMID: 38509985 Free PMC article.
-
Cellular and humoral immune responses to COVID-19 booster vaccination in Japanese dialysis patients.Clin Exp Nephrol. 2024 Jul;28(7):674-682. doi: 10.1007/s10157-024-02477-8. Epub 2024 Mar 8. Clin Exp Nephrol. 2024. PMID: 38457030
-
Incidence and Severity of COVID-19 in Relation to Anti-Receptor-Binding Domain IgG Antibody Level after COVID-19 Vaccination in Kidney Transplant Recipients.Viruses. 2024 Jan 12;16(1):114. doi: 10.3390/v16010114. Viruses. 2024. PMID: 38257814 Free PMC article.
-
Immune responses in COVID-19 patients: Insights into cytokine storms and adaptive immunity kinetics.Heliyon. 2024 Jul 14;10(14):e34577. doi: 10.1016/j.heliyon.2024.e34577. eCollection 2024 Jul 30. Heliyon. 2024. PMID: 39149061 Free PMC article. Review.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous