

Immunogenicity, safety, and efficacy of the HPV vaccines among people living with HIV: A systematic review and meta-analysis
- PMID: 35936024
- PMCID: PMC9350866
- DOI: 10.1016/j.eclinm.2022.101585
Immunogenicity, safety, and efficacy of the HPV vaccines among people living with HIV: A systematic review and meta-analysis
Abstract
Background: Vaccines have been demonstrated to protect against high-risk human papillomavirus infection (HPV), including HPV-16/18, and cervical lesions among HIV negative women. However, their efficacy remains uncertain for people living with HIV (PLHIV).We systematically reviewed available evidence on HPV vaccine on immunological, virological, or other biological outcomes in PLHIV.
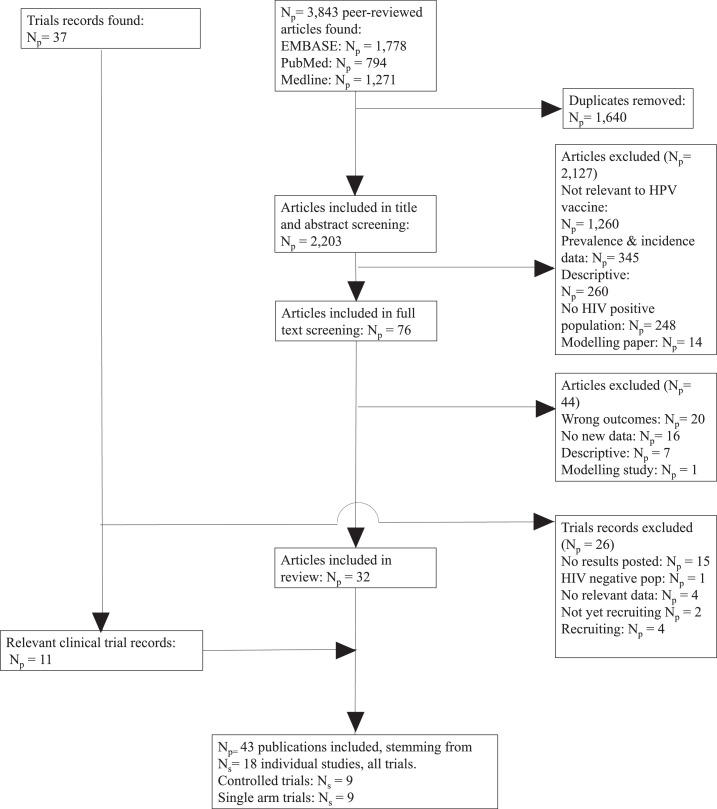
Methods: We searched five electronic databases (PubMed, Medline and Embase, clinicaltrials.gov and the WHO clinical trial database) for longitudinal prospective studies reporting immunogenicity, virological, cytological, histological, clinical or safety endpoints following prophylactic HPV vaccination among PLHIV. We included studies published by February 11th, 2021. We summarized results, assessed study quality, and conducted meta-analysis and subgroup analyses, where possible.
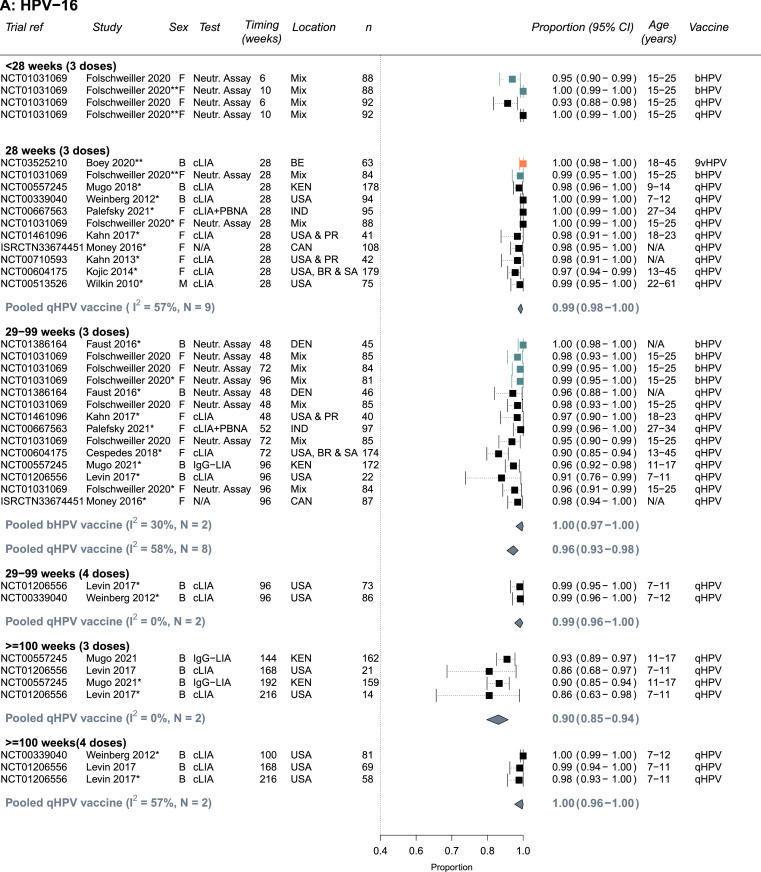
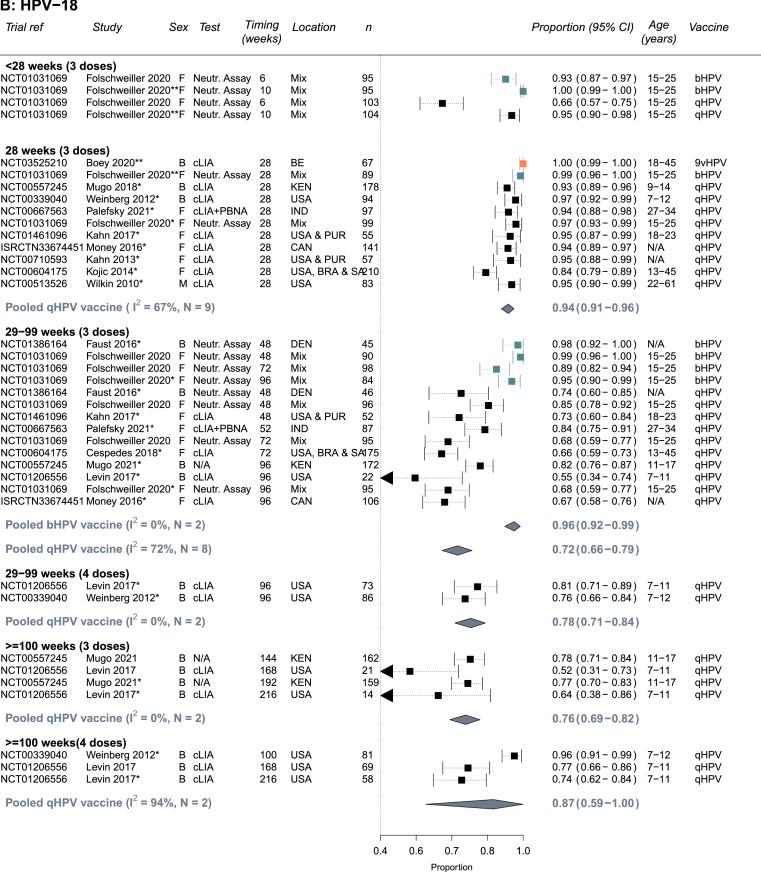
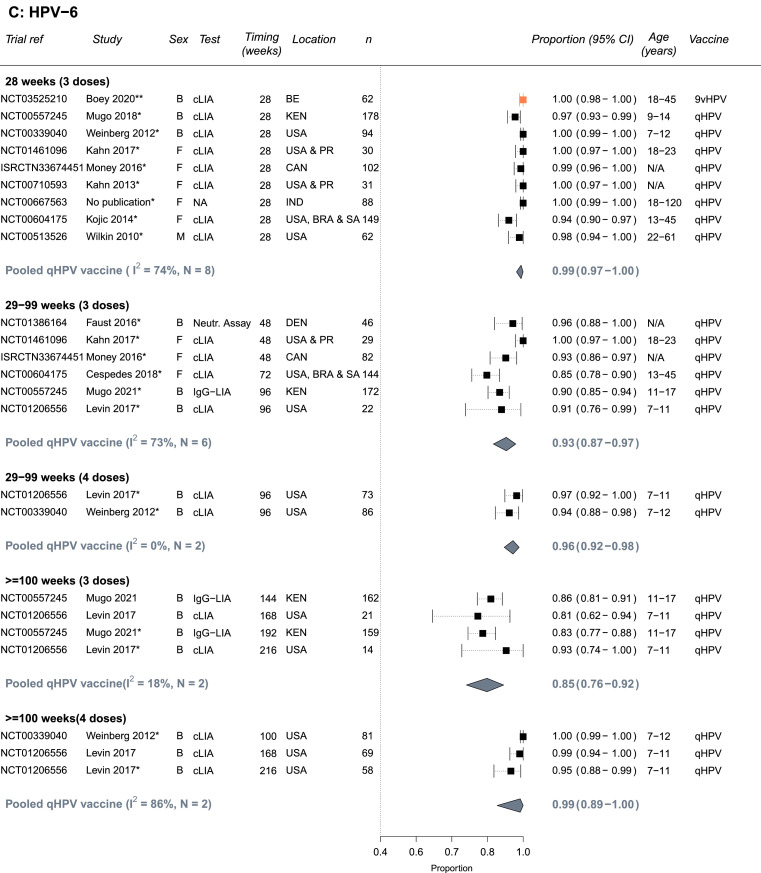
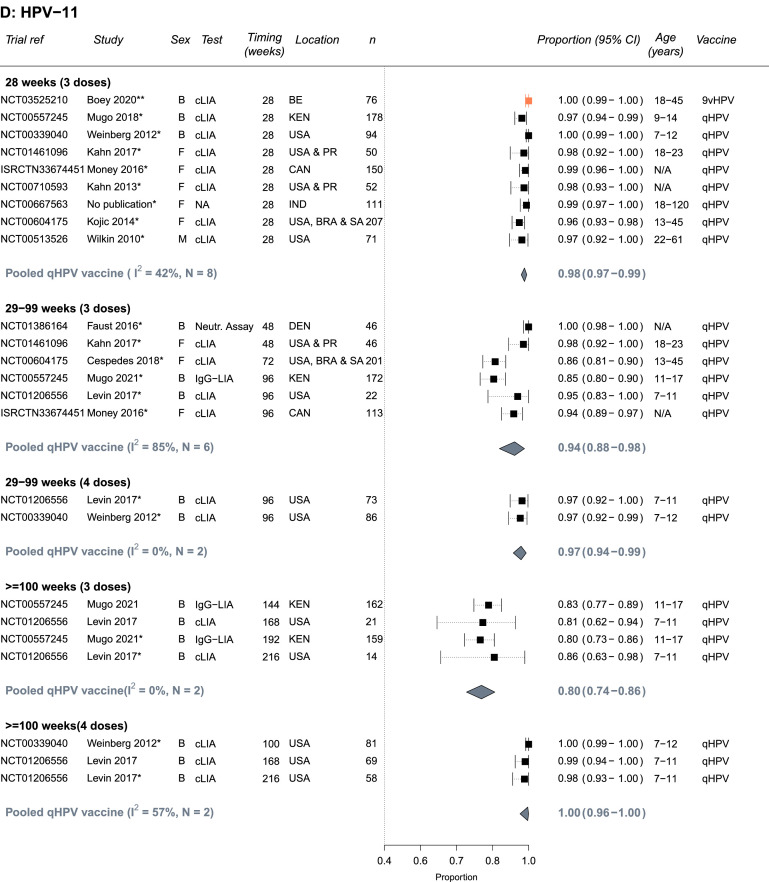
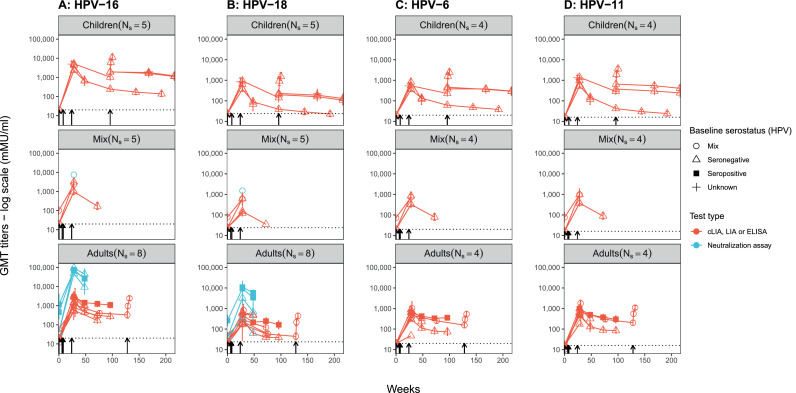
Findings: We identified 43 publications stemming from 18 independent studies (Ns =18), evaluating the quadrivalent (Ns =15), bivalent (Ns =4) and nonavalent (Ns =1) vaccines. A high proportion seroconverted for the HPV vaccine types. Pooled proportion seropositive by 28 weeks following 3 doses with the bivalent, quadrivalent, and nonavalent vaccines were 0.99 (95% confidence interval: 0.95-1.00, Ns =1), 0.99 (0.98-1.00, Ns =9), and 1.00 (0.99-1.00, Ns =1) for HPV-16 and 0.99 (0.96-1.00, Ns =1), 0.94 (0.91-0.96, Ns =9), and 1.00 (0.99-1.00, Ns =1) for HPV-18, respectively. Seropositivity remained high among people who received 3 doses despite some declines in antibody titers and lower seropositivity over time, especially for HPV-18, for the quadrivalent than the bivalent vaccine, and for HIV positive than negative individuals. Seropositivity for HPV-18 at 29-99 weeks among PLHIV was 0.72 (0.66-0.79, Ns =8) and 0.96 (0.92-0.99, Ns =2) after 3 doses of the quadrivalent and bivalent vaccine, respectively and 0.94 (0.90-0.98, Ns =3) among HIV-negative historical controls. Evidence suggests that the seropositivity after vaccination declines over time but it can lasts at least 2-4 years. The vaccines were deemed safe among PLHIV with few serious adverse events. Evidence of HPV vaccine efficacy against acquisition of HPV infection and/or associated disease from the eight trials available was inconclusive due to the low quality.
Interpretation: PLHIV have a robust and safe immune response to HPV vaccination. Antibody titers and seropositivity rates decline over time but remain high. The lack of a formal correlate of protection and efficacy results preclude definitive conclusions on the clinical benefits. Nevertheless, given the burden of HPV disease in PLHIV, although the protection may be shorter or less robust against HPV-18, the robust immune response suggests that PLHIV may benefit from receiving HPV vaccination after acquiring HIV. Better quality studies are needed to demonstrate the clinical efficacy among PLHIV.
Funding: World Health Organization. MRC Centre for Global Infectious Disease Analysis, Canadian Institutes of Health Research, UK Medical Research Council (MRC).
Keywords: Cervical cancer; HIV; Human papilloma virus; Meta-analysis; Vaccination.
© 2022 The Authors.
Conflict of interest statement
LS has received funding from Sanofi Pasteur/AstraZeneca outside of the submitted work. MMR reports funding from Charles A King Trust Postdoctoral Fellowship and Harvard Data Science Institute, and travel support to attend meetings for cervical cancer elimination from the WHO and Canadian Institute of Health Research, all outside of the submitted work. RVB received abstract and manuscript writing support from Regeneron Pharmaceuticals, outside the submitted work. MMG reports an investigator-sponsored research grant from Gilead Sciences Inc., and contractual arrangements from the Institut national de santé publique du Québec (INSPQ), the Institut d'excellence en santé et services sociaux (INESSS), the World Health Organization, and the Joint United Nations Programme on HIV/AIDS (UNAIDS), all outside of the submitted work. MB reports funding from Bill & Melinda Gates Foundation (grant number OPP48979), outside the submitted work.
Figures
Similar articles
-
Comparison of different human papillomavirus (HPV) vaccine types and dose schedules for prevention of HPV-related disease in females and males.Cochrane Database Syst Rev. 2019 Nov 22;2019(11):CD013479. doi: 10.1002/14651858.CD013479. Cochrane Database Syst Rev. 2019. PMID: 31755549 Free PMC article.
-
A systematic review of immunogenicity, clinical efficacy and safety of human papillomavirus vaccines in people living with the human immunodeficiency virus.Hum Vaccin Immunother. 2020;16(2):426-435. doi: 10.1080/21645515.2019.1656481. Epub 2019 Sep 20. Hum Vaccin Immunother. 2020. PMID: 31448991 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Human Papillomavirus Vaccine Efficacy and Effectiveness against Cancer.Vaccines (Basel). 2021 Nov 30;9(12):1413. doi: 10.3390/vaccines9121413. Vaccines (Basel). 2021. PMID: 34960159 Free PMC article. Review.
-
Efficacy, immunogenicity, and safety of a quadrivalent HPV vaccine in men: results of an open-label, long-term extension of a randomised, placebo-controlled, phase 3 trial.Lancet Infect Dis. 2022 Mar;22(3):413-425. doi: 10.1016/S1473-3099(21)00327-3. Epub 2021 Nov 12. Lancet Infect Dis. 2022. PMID: 34780705 Clinical Trial.
Cited by
-
Understanding human papillomavirus vaccine response and efficacy in people living with HIV: A systematic mixed studies review and meta-analysis.PLOS Glob Public Health. 2024 Dec 20;4(12):e0003931. doi: 10.1371/journal.pgph.0003931. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39705286 Free PMC article.
-
HPV Infection Profiles among People Living with HIV and HPV Vaccine Acceptance among Individuals with Different HIV Infection Statuses in China: A Systematic Meta-Analysis.Vaccines (Basel). 2023 Oct 19;11(10):1614. doi: 10.3390/vaccines11101614. Vaccines (Basel). 2023. PMID: 37897016 Free PMC article. Review.
-
The Assessment of Knowledge About Cervical Cancer, HPV Vaccinations, and Screening Programs Among Women as an Element of Cervical Cancer Prevention in Poland.J Pers Med. 2024 Dec 4;14(12):1139. doi: 10.3390/jpm14121139. J Pers Med. 2024. PMID: 39728052 Free PMC article.
-
High-risk human papillomavirus prevalence and serostatus in a cohort of cisgender women and people with a cervix living with perinatally acquired HIV.HIV Med. 2025 May;26(5):709-720. doi: 10.1111/hiv.70001. Epub 2025 Feb 25. HIV Med. 2025. PMID: 39999769 Free PMC article.
-
Human Papillomavirus Vaccination.N Engl J Med. 2023 May 11;388(19):1790-1798. doi: 10.1056/NEJMcp2108502. N Engl J Med. 2023. PMID: 37163625 Free PMC article. Review.
References
-
- Van de Velde N, Boily M-C, Drolet M, et al. Population-level impact of the bivalent, quadrivalent, and nonavalent human papillomavirus vaccines: a model–based analysis. JNCI J Natl Cancer Inst. 2012;104(22):1712–1723. - PubMed
-
- Cervical cancer. [cited 2022 Jan 19]. Available from: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer
-
- RIVM. Projected direct benefit of vaccination against HPV. [cited 2022 Feb 19]. Available from: https://www.rivm.nl/documenten/hpv-vaccination-in-netherlands
-
- PATH. Expanding access to HPV vaccines. [cited 2022 Feb 19]. Available from: https://www.path.org/media-center/expanding-access-hpv-vaccines-path-eva...
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
