

Comparison of Anterior vs. Dorsal Approach for Spinal Accessory to Suprascapular Nerve Transfer in Patients With a Brachial Plexus Injury and Its Outcome on Shoulder Function
- PMID: 35936186
- PMCID: PMC9346609
- DOI: 10.7759/cureus.26543
Comparison of Anterior vs. Dorsal Approach for Spinal Accessory to Suprascapular Nerve Transfer in Patients With a Brachial Plexus Injury and Its Outcome on Shoulder Function
Abstract
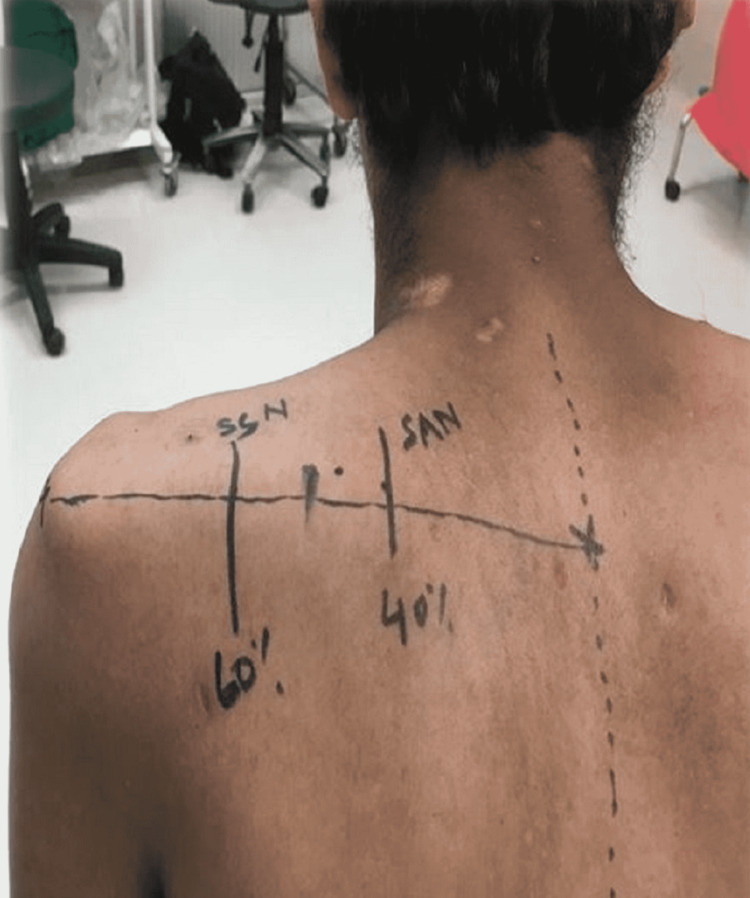
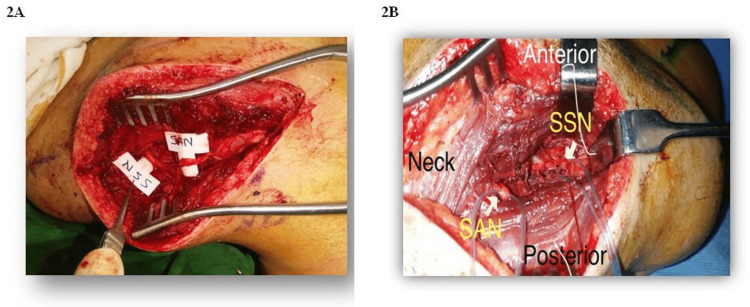
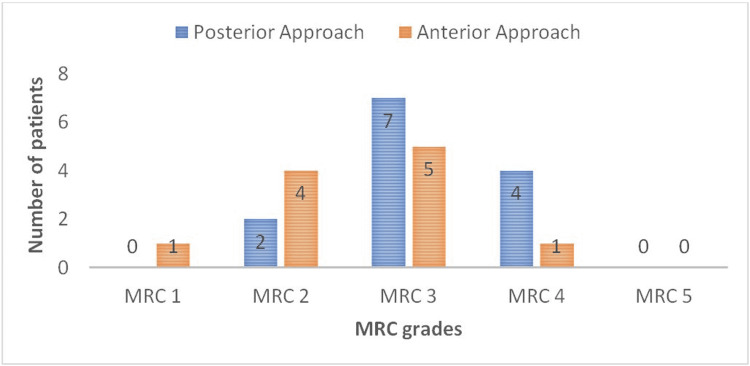
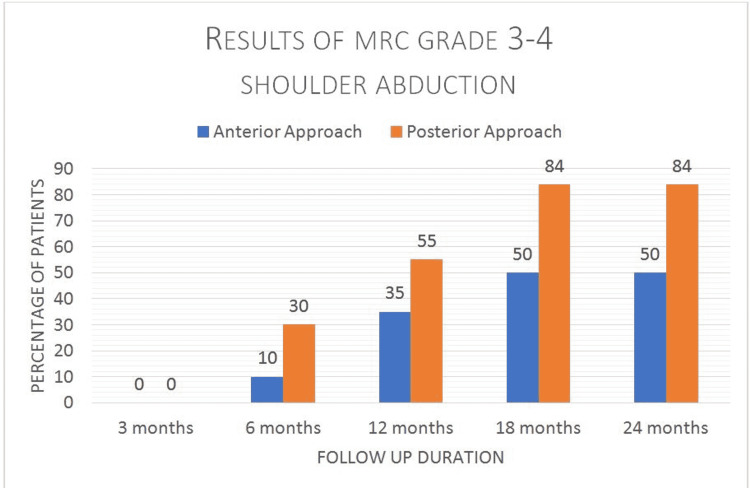
Background Brachial plexus injuries are frequently encountered in the domain of plastic surgery, mostly secondary to road traffic accidents, gunshot injuries, or falls from a height. Many modalities have been described in the management, depending on the level and duration of the injury. C5, C6 and C5, C6, C7 are two common patterns in which nerve repair and transfers are described. At our center, we practice spinal accessory to suprascapular nerve transfer in all patients with upper trunk brachial plexus injury. There are two described approaches for the spinal accessory nerve to suprascapular nerve transfer, i.e. anterior or dorsal. The rationale for doing the posterior approach is that this approach avoids damaging the suprascapular nerve at its entrance in the suprascapular notch under the suprascapular ligament during exploration due to traction. Materials and methods This is a retrospective study with a consecutive sampling of 23 patients presenting at Liaquat National Hospital, Karachi, with upper trunk brachial plexus injuries during the time period from January 2016 to December 2017, i.e. two years. We divided these 23 patients into two groups, one with the anterior approach and the other with a dorsal approach for spinal accessory to suprascapular nerve transfer for shoulder abduction. The mean duration of post-surgical follow-up was from 18 to 24 months and recovery and functional outcomes were assessed. Results Out of the 23 patients that were included, 10 patients were operated on with an anterior approach and 13 with a posterior approach. Fifty percent (50%) of patients operated with the anterior approach and 84% of patients with the posterior showed the best motor grade recovery of M4, respectively, with better performance in patients with the posterior approach as compared to the anterior approach. Conclusion We advocate taking a posterior approach for spinal accessory to suprascapular nerve transfer for shoulder abduction, as it has shown better results with reliable outcomes concerning shoulder abduction, angle of abduction, and range of motion.
Keywords: anterior approach; bilateral brachial plexus injury; dorsal approach; nerve transfer; shoulder function; spinal accessory nerve; suprascapular nerve.
Copyright © 2022, Tahir et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Long-term clinical outcomes of spinal accessory nerve transfer to the suprascapular nerve in patients with brachial plexus palsy.Acta Neurochir (Wien). 2016 Sep;158(9):1801-6. doi: 10.1007/s00701-016-2886-1. Epub 2016 Jul 7. Acta Neurochir (Wien). 2016. PMID: 27383201
-
Spinal Accessory to Suprascapular Nerve Transfer in Traumatic Brachial Plexus Injury: A Comparative Study of Shoulder Recovery Outcomes in the Anterior versus Posterior Approach and Surgeons' Preference.World Neurosurg. 2024 Sep;189:e970-e976. doi: 10.1016/j.wneu.2024.07.056. Epub 2024 Jul 14. World Neurosurg. 2024. PMID: 39004182
-
Results of spinal accessory to suprascapular nerve transfer in 110 patients with complete palsy of the brachial plexus.J Neurosurg Spine. 2016 Jun;24(6):990-5. doi: 10.3171/2015.8.SPINE15434. Epub 2016 Feb 12. J Neurosurg Spine. 2016. PMID: 26871649
-
The extent of brachial plexus injury: an important factor in spinal accessory nerve to suprascapular nerve transfer outcomes.Br J Neurosurg. 2020 Oct;34(5):591-594. doi: 10.1080/02688697.2019.1639620. Epub 2019 Jul 15. Br J Neurosurg. 2020. PMID: 31307250
-
[Paralytic shoulder secondary to post-traumatic peripheral nerve lesions in the adult].Acta Orthop Belg. 1999 Mar;65(1):10-22. Acta Orthop Belg. 1999. PMID: 10216997 Review. French.
Cited by
-
The trapezius plane block: Extended use in perioperative pain management in nerve transfer surgeries.Saudi J Anaesth. 2024 Jul-Sep;18(3):435-437. doi: 10.4103/sja.sja_3_24. Epub 2024 Jun 4. Saudi J Anaesth. 2024. PMID: 39149743 Free PMC article.
-
Spinal Accessory Nerve to Suprascapular Nerve Transfer by Dorsal Approach for Shoulder Reanimation in Cases of Brachial Plexus Injuries: Surgical Technique.Indian J Plast Surg. 2024 Jun 21;57(5):350-355. doi: 10.1055/s-0044-1786767. eCollection 2024 Oct. Indian J Plast Surg. 2024. PMID: 39552801 Free PMC article. Review.
References
-
- Functional outcome predictors after spinal accessory nerve to suprascapular nerve transfer for restoration of shoulder abduction in traumatic brachial plexus injuries in adults: the effect of time from injury to surgery. Solla DJ, de Oliveira AJ, Riechelmann RS, Martins RS, Siqueira MG. https://link.springer.com/article/10.1007/s00068-020-01501-2. Eur J Trauma Emerg Surg. 2022;48:1217–1223. - PubMed
-
- Outcomes of spinal accessory-to-suprascapular nerve transfers for brachial plexus birth injury. Segal D, Cornwall R, Little KJ. J Hand Surg Am. 2019;44:578–587. - PubMed
-
- The epidemiology of adult traumatic brachial plexus lesions in a large metropolis. Faglioni W Jr, Siqueira MG, Martins RS, Heise CO, Foroni L. https://link.springer.com/article/10.1007/s00701-013-1948-x. Acta Neurochir (Wien) 2014;156:1025–1028. - PubMed
-
- Timing of surgery in traumatic brachial plexus injury: a systematic review. Martin E, Senders JT, DiRisio AC, Smith TR, Broekman ML. J Neurosurg. 2018;130:1–13. - PubMed
-
- Monitoring to prevent brachial plexus injury. Thatte MR. https://jpgmonline.com/article.asp?issn=0022-3859;year=2014;volume=60;is.... J Postgrad Med. 2014;60:241–242. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous