

Ten-Year Review of Gestational Trophoblastic Disease at Lady Reading Hospital, Peshawar
- PMID: 35936190
- PMCID: PMC9356217
- DOI: 10.7759/cureus.26620
Ten-Year Review of Gestational Trophoblastic Disease at Lady Reading Hospital, Peshawar
Abstract
Objective: To determine the frequency and management outcome of gestational trophoblastic disease (GTD) in Lady Reading Hospital.
Methods: This was a retrospective observational study at Lady Reading Hospital, Peshawar, from January 2011 to December 2021. Hospital records of all patients with GTD were reviewed and all were included in this study except those with an incomplete record or unconfirmed histology. Treatment was analysed in terms of surgical, chemotherapy or no treatment, and outcomes were noted in terms of complete remission, disease persistence or death.
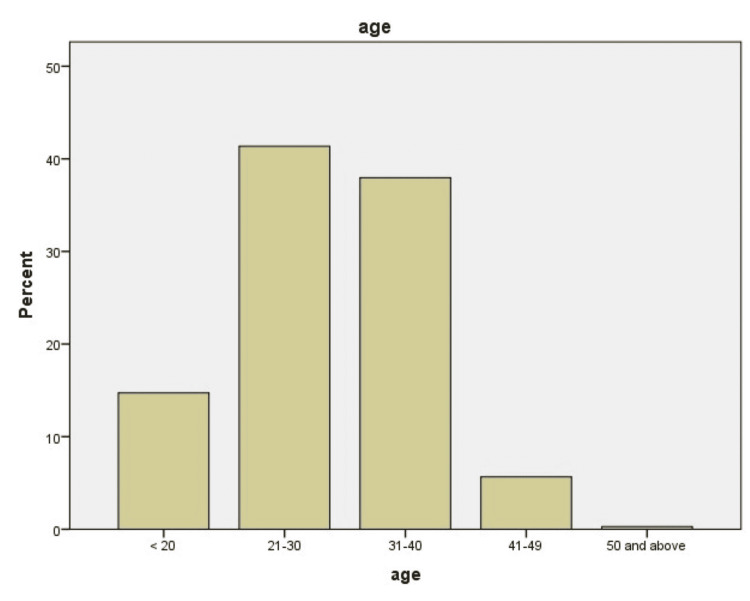
Results: In 10 years 353 patients were admitted with GTD, and the frequency of the disease was 3.72 cases per 1000 pregnancies. The most frequent lesions were complete mole 65.2% (n=230) followed by invasive mole 20.4% (n=72). Mortality rate was 0.56% (n=2). Maternal blood group analysis revealed that B positive 28.3% (n=100) was more frequent. O positive blood group was found more in the malignant form of the disease at 3.96% (n=14). GTD was most prevalent in 21 to 30 years of age (41.4%, n=146). Regarding treatment, in 69.97% (n=247) of cases, suction and evacuation were performed, in 4.2% (n=15) of cases hysterectomy was performed as primary therapy, and 4.8% (17) needed hysterectomy for chemoresistance. In this study 42.49% (n=150) were given single-agent chemotherapy and 4.8% (n=17) were given multi-agent therapy. We had 21.33% (32) patients with a risk score of 7-9. In the group with a risk score of 7-9, 15.62% (n=5) patients were directly started on multi-agent therapy because of evidence of metastasis or choriocarcinoma; the remaining 84.37% (n=27) of patients who had no evidence of metastasis, no prior chemotherapy, no choriocarcinoma and International Federation of Obstetrics and Gynecology (FIGO) stage 1 were given single-agent methotrexate with folinic acid (eight days) after informed consent. In 18.75% of patients (n=6) hysterectomy was performed as the primary treatment either for haemorrhage or with age > 40, family completed, or reluctance to undergo chemotherapy. They all had a complete cure. In 3.1% (n=1) of cases, resistance to single-agent therapy was found and multi-agent treatment was started. Overall, in 96.29% of patients, complete remission was achieved with single-agent therapy in patients with risk scores of 7-9.
Conclusion: The frequency of GTD was 3.4/1000 pregnancies. Complete mole was the most frequent lesion, and single-agent chemotherapy had a good outcome in low- and high-risk patients with a risk score of 7-9 (with no evidence of metastasis, prior chemotherapy, or choriocarcinoma and FIGO stage 1).
Keywords: choriocarcinoma; complete mole; gestational trophoblastic neoplasia; hydatiform mole; s: gestational trophoblastic disease.
Copyright © 2022, Hussain et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Predictors for single-agent resistance in FIGO score 5 or 6 gestational trophoblastic neoplasia: a multicentre, retrospective, cohort study.Lancet Oncol. 2021 Aug;22(8):1188-1198. doi: 10.1016/S1470-2045(21)00262-X. Epub 2021 Jun 25. Lancet Oncol. 2021. PMID: 34181884
-
Management of postmolar gestational trophoblastic disease with methotrexate and folinic acid: 15 years of experience.J Reprod Med. 2006 Oct;51(10):835-40. J Reprod Med. 2006. PMID: 17086813
-
Gestational trophoblastic neoplasia after human chorionic gonadotropin normalization in a retrospective cohort of 7761 patients in France.Am J Obstet Gynecol. 2021 Oct;225(4):401.e1-401.e9. doi: 10.1016/j.ajog.2021.05.006. Epub 2021 May 18. Am J Obstet Gynecol. 2021. PMID: 34019886
-
Guideline No. 408: Management of Gestational Trophoblastic Diseases.J Obstet Gynaecol Can. 2021 Jan;43(1):91-105.e1. doi: 10.1016/j.jogc.2020.03.001. J Obstet Gynaecol Can. 2021. PMID: 33384141 Review.
-
Diagnosis and Management of Gestational Trophoblastic Disease: A Comparative Review of National and International Guidelines.Obstet Gynecol Surv. 2020 Dec;75(12):747-756. doi: 10.1097/OGX.0000000000000848. Obstet Gynecol Surv. 2020. PMID: 33369685 Review.
References
-
- Gestational trophoblastic disease in the Asian population of Northern England and North Wales. Tham BW, Everard JE, Tidy JA, et al. Int J Obstet Gynaecol. 2003;110:555–559. - PubMed
-
- Gestational trophoblastic disease: experience at Nawabshah Hospital. Nizam K, Haider G, Memon N, et al. https://pubmed.ncbi.nlm.nih.gov/20364752/ J Ayub Med Coll Abbottabad. 2009;21:94–97. - PubMed
-
- Gestational trophoblastic neoplasia management: an update. Ngan S, Seckl MJ. Curr Opin Oncol. 2007;19:486–491. - PubMed
LinkOut - more resources
Full Text Sources