

Exercise-Diet Therapy Combined with Insulin Aspart Injection for the Treatment of Gestational Diabetes Mellitus: A Study on Clinical Effect and Its Impact
- PMID: 35936373
- PMCID: PMC9352494
- DOI: 10.1155/2022/4882061
Exercise-Diet Therapy Combined with Insulin Aspart Injection for the Treatment of Gestational Diabetes Mellitus: A Study on Clinical Effect and Its Impact
Abstract
Objective: To explore the clinical effect and impact of exercise-diet therapy combined with Insulin Aspart Injection on gestational diabetes mellitus (GDM).
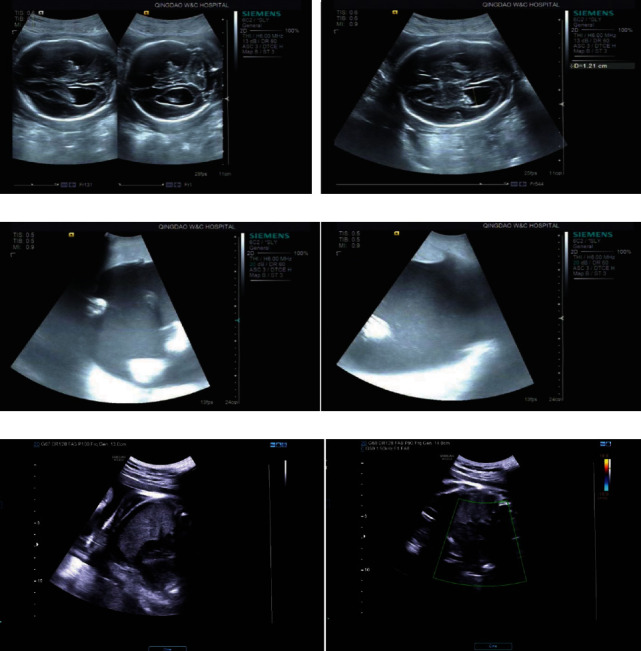
Methods: The objects of study were patients with pregestational diabetes mellitus (PGDM) and 62 patients with GDM who were diagnosed by oral glucose tolerance test (OGTT) and insulin release test from February 2017 to February 2019. According to the severity of the disease, enrolled patients were informed to have appropriate exercise and diet control or Insulin Aspart Injection on this basis until the completion of delivery. By using 50 pregnant women with normal glucose as the control, the fasting plasma glucose (FPG), 1-hour postprandial glucose (1hPG), 2-hour postprandial glucose (2hPG), nocturnal glucose, and glycosylated hemoglobin (HbA1c) levels were compared between the PGDM group and the GDM group before and after treatment; besides, further comparison was made in terms of glucose compliance rate, islet B-cell secretory function, and insulin resistance after treatment. The pregnant women were examined by B-ultrasound at 24 and 26 weeks of gestation to check if the fetus had abnormalities in the central nervous system and the heart. Further B-ultrasound examination was performed at 32 and 37 weeks of gestation to check the problems such as polyhydramnios and stillbirth. In addition, a comparative analysis was carried out in terms of the adverse pregnancy outcomes and complications, associated with the comparison of the results after treatment with control group.
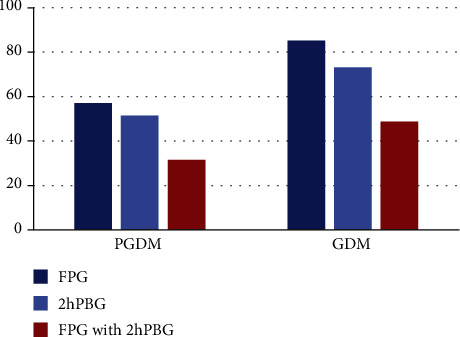
Results: After treatment, the levels of FPG, 1hPG, 2hPG, nocturnal glucose, and HbA1c were decreased in the PGDM group and GDM group than those before treatment, especially in the GDM group, with significant difference still when compared with the control group (P < 0.05). Statistical analysis revealed that the blood glucose compliance rate in the GDM group was higher than that in the PGDM group, showing a better therapeutic effect. Fasting insulin (FINS) and homeostasis model assessment index for insulin resistance (HOMA-IR) in the GDM group were significantly higher than those in control group, but lower than those in the PGDM group (P < 0.01), while the level of HOMA-β was lower in the GDM group than that in the control group and higher than that in PGDM (P < 0.01). Further ultrasound examination revealed the presence of fetal cardiac abnormality, polyhydramnios, stillbirth, and problems, showing a higher incidence in the PGDM group but almost nonexistence in the control group. In addition, the incidence of hypertension, macrosomia, premature rupture of membranes, postpartum hemorrhage, and infection were obviously higher in the PGDM group than those in the GDM group and control group (P < 0.05).
Conclusion: Exercise-diet therapy combined with Insulin Aspart Injection can effectively control the blood glucose level of pregnant patients with GDM, improve the pregnancy outcome to a certain extent, and ensure the health of pregnant women and fetus, which is worthy of clinical application.
Copyright © 2022 Amei Mu et al.
Conflict of interest statement
The authors declare that they do not have any commercial or associative interest that represents a conflict of interest in connection with the work submitted.
Figures
Similar articles
-
Use of oral glucose tolerance testing and HbA1c at 6-14 gestational weeks to predict gestational diabetes mellitus in high-risk women.Arch Gynecol Obstet. 2023 May;307(5):1451-1457. doi: 10.1007/s00404-022-06637-7. Epub 2022 Jun 7. Arch Gynecol Obstet. 2023. PMID: 35670847
-
[Investigation of pregestational diabetes mellitus in 15 hospitals in Guangdong province].Zhonghua Fu Chan Ke Za Zhi. 2017 Jul 25;52(7):436-442. doi: 10.3760/cma.j.issn.0529-567X.2017.07.002. Zhonghua Fu Chan Ke Za Zhi. 2017. PMID: 28797149 Chinese.
-
Report of the Committee on the classification and diagnostic criteria of diabetes mellitus.Diabetes Res Clin Pract. 2002 Jan;55(1):65-85. doi: 10.1016/s0168-8227(01)00365-5. Diabetes Res Clin Pract. 2002. PMID: 11755481
-
Characteristics and pregnancy outcomes of subtypes of gestational diabetes mellitus based on HOMA-IR and BMI.Arch Gynecol Obstet. 2024 Nov;310(5):2355-2361. doi: 10.1007/s00404-024-07733-6. Epub 2024 Sep 17. Arch Gynecol Obstet. 2024. PMID: 39287682 Review.
-
[Gestational diabetes mellitus (Update 2019)].Wien Klin Wochenschr. 2019 May;131(Suppl 1):91-102. doi: 10.1007/s00508-018-1419-8. Wien Klin Wochenschr. 2019. PMID: 30980150 Review. German.
Cited by
-
Insulin aspart plus high-dose vitamin D supplementation for gestational diabetes mellitus: analysis of efficacy and risk factors for maternal and infant outcomes.Am J Transl Res. 2024 Aug 15;16(8):4200-4207. doi: 10.62347/PKAY4284. eCollection 2024. Am J Transl Res. 2024. PMID: 39262735 Free PMC article.
-
Advanced maternal age, overweight and obese positively correlate to the abnormal plasma glucose among gestational diabetes mellitus women even with physical exercise > 90 min/day: a prospective cohort study in Shanghai.Sci Rep. 2025 Jul 1;15(1):21191. doi: 10.1038/s41598-025-09097-6. Sci Rep. 2025. PMID: 40594962 Free PMC article.
-
Effects of insulin aspart and metformin on gestational diabetes mellitus and inflammatory markers.World J Diabetes. 2023 Oct 15;14(10):1532-1540. doi: 10.4239/wjd.v14.i10.1532. World J Diabetes. 2023. PMID: 37970132 Free PMC article.
References
-
- Subiabre M., Silva L., Toledo F., et al. Insulin therapy and its consequences for the mother, foetus, and newborn in gestational diabetes mellitus. Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease . 2018;1864(9):2949–2956. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
