

Evaluation of Hybrid VMAT Advantages and Robustness Considering Setup Errors Using Surface Guided Dose Accumulation for Internal Lymph Mammary Nodes Irradiation of Postmastectomy Radiotherapy
- PMID: 35936730
- PMCID: PMC9354548
- DOI: 10.3389/fonc.2022.907181
Evaluation of Hybrid VMAT Advantages and Robustness Considering Setup Errors Using Surface Guided Dose Accumulation for Internal Lymph Mammary Nodes Irradiation of Postmastectomy Radiotherapy
Abstract
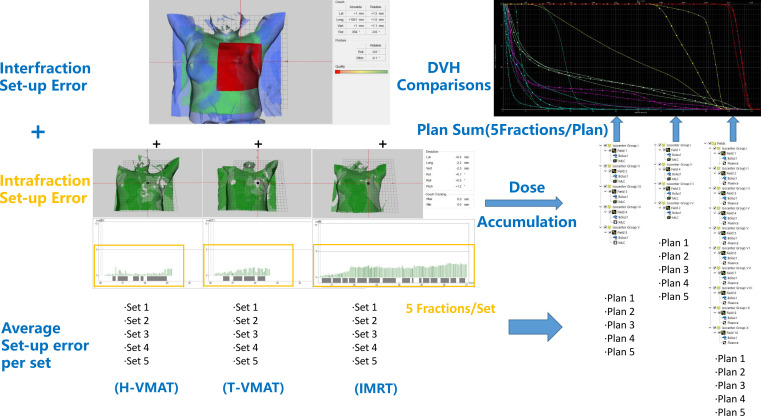
Objectives: Setup error is a key factor affecting postmastectomy radiotherapy (PMRT) and irradiation of the internal mammary lymph nodes is the most investigated aspect for PMRT patients. In this study, we evaluated the robustness, radiobiological, and dosimetric benefits of the hybrid volumetric modulated arc therapy (H-VMAT) planning technique based on the setup error in dose accumulation using a surface-guided system for radiation therapy.
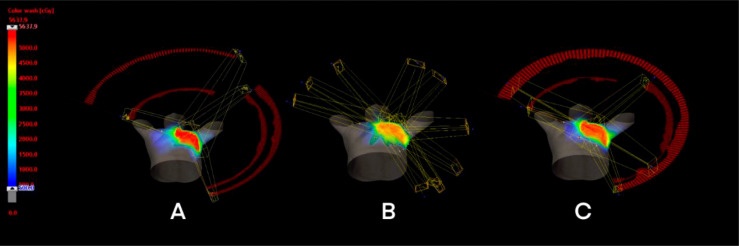
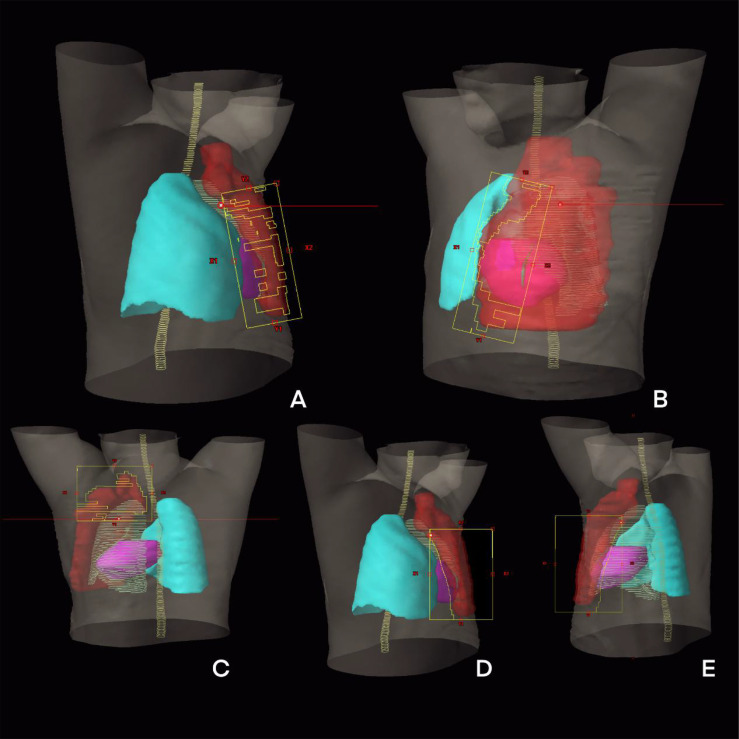
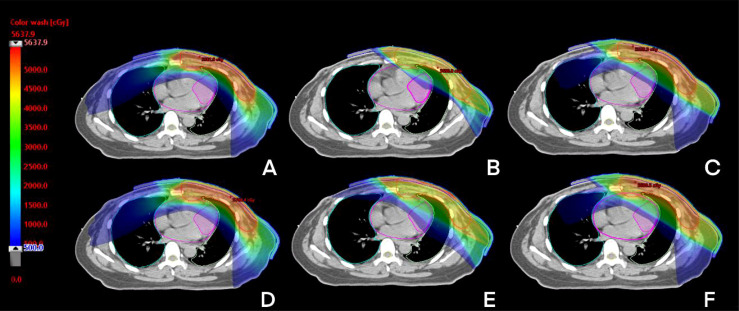
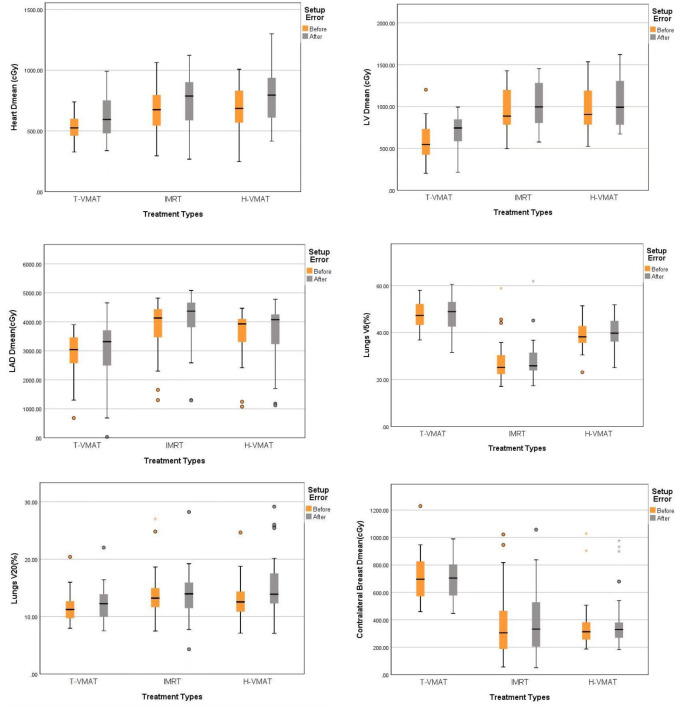
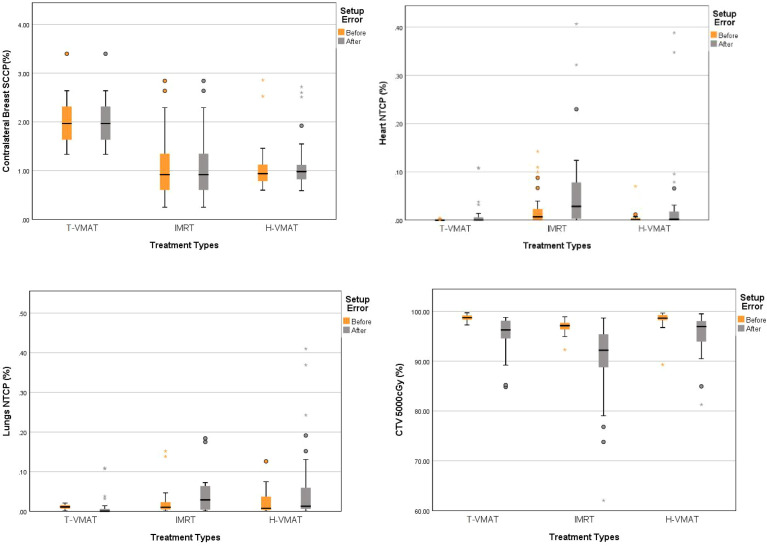
Methods: We retrospectively selected 32 patients treated by a radiation oncologist and evaluated the clinical target volume (CTV), including internal lymph node irradiation (IMNIs), and considered the planning target volume (PTV) margin to be 5 mm. Three different planning techniques were evaluated: tangential-VMAT (T-VMAT), intensity-modulated radiation therapy (IMRT), and H-VMAT. The interfraction and intrafraction setup errors were analyzed in each field and the accumulated dose was evaluated as the patients underwent daily surface-guided monitoring. These parameters were included while evaluating CTV coverage, the dose required for the left anterior descending artery (LAD) and the left ventricle (LV), the normal tissue complication probability (NTCP) for the heart and lungs, and the second cancer complication probability (SCCP) for contralateral breast (CB).
Results: When the setup error was accounted for dose accumulation, T-VMAT (95.51%) and H-VMAT (95.48%) had a higher CTV coverage than IMRT (91.25%). In the NTCP for the heart, H-VMAT (0.04%) was higher than T-VMAT (0.01%) and lower than IMRT (0.2%). However, the SCCP (1.05%) of CB using H-VMAT was lower than that using T-VMAT (2%) as well as delivery efficiency. And T-VMAT (3.72) and IMRT (10.5).had higher plan complexity than H-VMAT (3.71).
Conclusions: In this study, based on the dose accumulation of setup error for patients with left-sided PMRT with IMNI, we found that the H-VMAT technique was superior for achieving an optimum balance between target coverage, OAR dose, complication probability, plan robustness, and complexity.
Keywords: H-VMAT; IMNIs; PMRT; SGRT; biological models; setup error.
Copyright © 2022 Zhang, Li, Peng, Tan, Yang, Peng, Li, Qi, Sun, Liu and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A dosimetric and radiobiological evaluation of VMAT following mastectomy for patients with left-sided breast cancer.Radiat Oncol. 2021 Sep 6;16(1):171. doi: 10.1186/s13014-021-01895-2. Radiat Oncol. 2021. PMID: 34488817 Free PMC article.
-
Evaluation of a mixed beam therapy for postmastectomy breast cancer patients: Bolus electron conformal therapy combined with intensity modulated photon radiotherapy and volumetric modulated photon arc therapy.Med Phys. 2018 Jul;45(7):2912-2924. doi: 10.1002/mp.12958. Epub 2018 May 27. Med Phys. 2018. PMID: 29749075 Free PMC article.
-
Left breast irradiation with tangential intensity modulated radiotherapy (t-IMRT) versus tangential volumetric modulated arc therapy (t-VMAT): trade-offs between secondary cancer induction risk and optimal target coverage.Radiat Oncol. 2019 Sep 2;14(1):156. doi: 10.1186/s13014-019-1363-4. Radiat Oncol. 2019. PMID: 31477165 Free PMC article.
-
Volumetric arc therapy: A viable option for right-sided breast with comprehensive regional nodal irradiation in conjunction with deep inspiration breath hold.J Med Imaging Radiat Sci. 2021 Jun;52(2):223-237. doi: 10.1016/j.jmir.2021.02.007. Epub 2021 Mar 23. J Med Imaging Radiat Sci. 2021. PMID: 33771509
-
Robust optimization in lung treatment plans accounting for geometric uncertainty.J Appl Clin Med Phys. 2018 May;19(3):19-26. doi: 10.1002/acm2.12291. Epub 2018 Mar 10. J Appl Clin Med Phys. 2018. PMID: 29524301 Free PMC article. Review.
Cited by
-
Hybrid Treatment Planning for Chest Wall Irradiation Utilizing Three-Dimensional Conformal Radiotherapy (3DCRT), Intensity-Modulated Radiation Therapy (IMRT), and Volumetric Modulated Arc Therapy (VMAT): A Systematic Review.Cureus. 2024 May 3;16(5):e59583. doi: 10.7759/cureus.59583. eCollection 2024 May. Cureus. 2024. PMID: 38832195 Free PMC article. Review.
-
Comparative Study of Plan Robustness for Breast Radiotherapy: Volumetric Modulated Arc Therapy Plans with Robust Optimization versus Manual Flash Approach.Diagnostics (Basel). 2023 Nov 7;13(22):3395. doi: 10.3390/diagnostics13223395. Diagnostics (Basel). 2023. PMID: 37998531 Free PMC article.
-
Why is Volumetric Modulated Arc Therapy Not Considered the Standard of Care for Locoregional Radiation Therapy for Breast Cancer Patients?Adv Radiat Oncol. 2025 Jan 27;10(5):101728. doi: 10.1016/j.adro.2025.101728. eCollection 2025 May. Adv Radiat Oncol. 2025. PMID: 40264855 Free PMC article.
-
Dosimetric and Radiobiological Impact of Patient Setup Errors in Intensity-modulated Radiotherapy for Esophageal Cancer.Technol Cancer Res Treat. 2025 Jan-Dec;24:15330338241311136. doi: 10.1177/15330338241311136. Technol Cancer Res Treat. 2025. PMID: 39840692 Free PMC article.
References
-
- Quirk S, Grendarova P, Phan T, Conroy L, Burke B, Long K, et al. . A Retrospective Multi-Institutional Analysis to Define Dosimetric Recommendations for the Left Anterior Descending Artery for Left-Sided Breast Cancer Patients Treated With Radiotherapy. RadiotheR Oncol (2020). doi: 10.1016/j.radonc.2020.04.022 - DOI - PubMed
-
- Gagliardi G, Bjohle J, Lax I, Ottolenghi A, Eriksson F, Liedberg A, et al. . Radiation Pneumonitis After Breast Cancer Irradiation: Analysis of the Complication Probability Using the Relative Seriality Model. Int J Radiat Oncol Biol Phys (2000) 46:373–81. doi: 10.1016/S0360-3016(99)00420-4 - DOI - PubMed
LinkOut - more resources
Full Text Sources