

doi: 10.1016/j.eats.2022.03.012.
eCollection 2022 Jul.
Arthroscopic Scaphocapitate Fusion: Surgical Technique
Affiliations
- PMID: 35936845
- PMCID: PMC9353331
- DOI: 10.1016/j.eats.2022.03.012
Item in Clipboard
Arthroscopic Scaphocapitate Fusion: Surgical Technique
Arthrosc Tech.
.
Abstract
Scapholunate fusion appears to be an interesting surgical solution for carpal pathologies, which are sometimes difficult to manage as Kienbock's disease or chronic scapholunate instability. Open intracarpal fusion is notorious for decreasing joint range of motion due to the fusion of several carpal bones and because of the capsulotomy sectioning important ligamentous elements in carpal biomechanics. Wrist arthroscopy has already demonstrated its effectiveness in preserving joint mobility compared with open procedures. In this work, we present a detailed procedure for performing a scaphocapitate fusion under arthroscopy by specifying the key points of this procedure in our experience.
© 2022 The Authors.
Figures

Midcarpal arthroscopic view through the radial midcarpal portal. The patient’s arm is secured to the arm board, and Chinese fingers traps are used to apply 5–7 kg (11–15.5 lb) of traction along the arm’s axis vertically. This is an arthroscopic view with the optic positioned through the RMC portal. We observe the articular surfaces of the capitate and scaphoid, showing that chondromalacia has already evolved. The head of the capitate (top) appears to be devoid of its cartilage as well as the scaphoid surface (bottom).
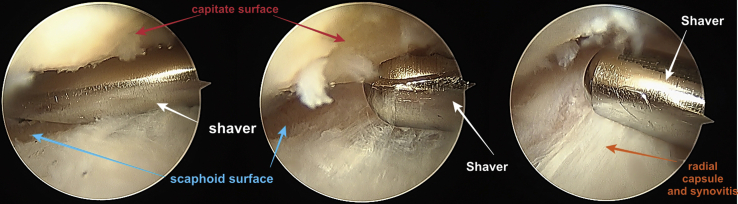
Large synovectomy and superficial bone debridement, arthroscopic view through the radial midcarpal portal (optic) and the use of a shaver through the ulnar midcarpal portal. It is essential to perform the widest possible synovectomy because the scaphocapitate space is narrow (left and center). The space must be cleared and widened (especially at the level of the joint capsule) to allow a better passage of the instruments (right).
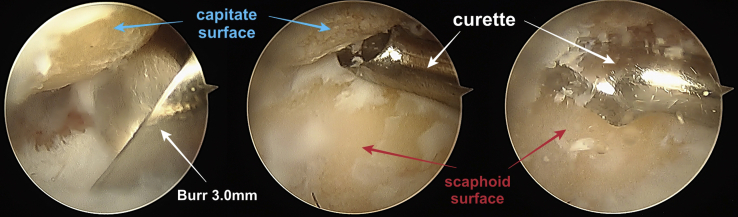
Scaphocapitate bone debridement with an arthroscopic view through the ulnar midcarpal portal (optic) and the use of a 3-mm burr (left) and a curette (center) through the radial midcarpal portal. Debridement should be vigorous until a bloody dew appears. Very often, during bone debridement in a humid environment, a "snowstorm" effect (right) may appear which may compromise arthroscopic visibility in such a narrow space. We recommend the use of numerous washouts, as well as alternating between wet and dry arthroscopy.
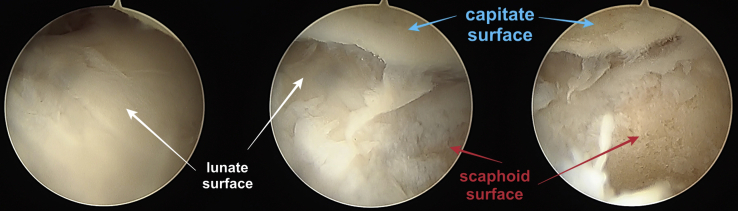
Midcarpal arthroscopic exploration after bone debridement through ulnar midcarpal portal. On the left, we can see that the cartilage of the lunate is intact. The image on the right shows the absence of cartilage on the articular surfaces of the capitate and the scaphoid. The image in the center shows us all the midcarpal articular surfaces of the three mentioned bones.

Appearance of a “bloody dew” during excision of the cartilage and milling of the subchondral bone during an arthroscopic view through the radial midcarpal approach. The appearance of this bloody dew is a sign of sufficient swelling for good bone healing. The appearance of bloody dew can be seen even when the tourniquet is inflated.

Arthroscopic wash-out (optic through ulnar midcarpal portal). In the case of major joint debridement, a lot of joint debris can impede visibility and be difficult to remove because there is so much of it. One trick is to remove the drill from its cannula and then introduce the cannula into the joint in wet arthroscopy. The suction system left in place allows the bone debris floating in the irrigation fluid to be sucked up and removed, and larger debris to be removed with forceps.

(A) Insertion of the bone graft into several 20-gauge needle plugs (intramuscular). The ends of the plugs are cut in a bevel shape for better insertion into arthroscopic passages. (B) Once introduced through the midcarpal radial portal, the bone graft is then pushed into the joint using the introducer. (C) Arthroscopic control is used to ensure the correct positioning of the bone graft during its introduction.

Three-month postoperative CT scan with coronal reconstructions (A and B) and 3D reconstruction (C) for a scaphocapitate fusion due to iatrogenic damage to the capitate cartilage after scaphoid pseudarthrosis. Note here that the addition of a longitudinal screw in the axis of the scaphoid due to the initial scaphoid pseudarthrosis. In A, we can see the screw breaking into the capitate-hamate joint, probably due to an underestimation of the compression effect. However, due to the almost zero mobility of this joint, the patient was symptom-free.
References
-
- Arianni M., Mathoulin C. Arthroscopic interposition tendon arthroplasty for stage 2 scapholunate advanced collapse. Arthroscopy. 2019;35:392–402. - PubMed
-
- Wu C.H., Strauch R.J. Wrist denervation. Orthop Clin NA. 2019;50:345–356. - PubMed
-
- Delétang F., Segret J., Dap F., Dautel G. Chronic scapholunate instability treated by scaphocapitate fusion: A midterm outcome perspective. Orthop Traumatol Surg Res. 2011;97:164–171. - PubMed
-
- Collon S., Tham S.K.Y., McCombe D., Bacle G. Scaphocapitate fusion for the treatment of Lichtman stage III Kienböck’s disease. Results of a single center study with literature review. Hand Surg Rehabil. 2020;39:201–206. - PubMed
LinkOut - more resources
Full Text Sources
