

doi: 10.1016/j.eats.2022.02.031.
eCollection 2022 Jul.
The Lark Loop Used for Proximal Biceps Tenodesis: An All-Arthroscopic Technique
Affiliations
- PMID: 35936850
- PMCID: PMC9353156
- DOI: 10.1016/j.eats.2022.02.031
Item in Clipboard
The Lark Loop Used for Proximal Biceps Tenodesis: An All-Arthroscopic Technique
Arthrosc Tech.
.
Abstract
Long head of the biceps tendinopathy is a common shoulder problem that is difficult to diagnose and treat. Biceps tenodesis is an effective surgical approach target for long head of the biceps tendon lesions. This article describes an all-arthroscopic proximal biceps tenodesis technique. This technique uses a high-strength suture to construct a tear-resistant loop; fixation is achieved with a suture anchor at the proximal aspect of the intertubercular groove or the greater tuberosity. This tenodesis fixation is simple, with no neurovascular injury or humeral fracture risk. In addition, our technique is cost-effective, with no need for specialty sutures.
© 2022 The Authors.
Figures
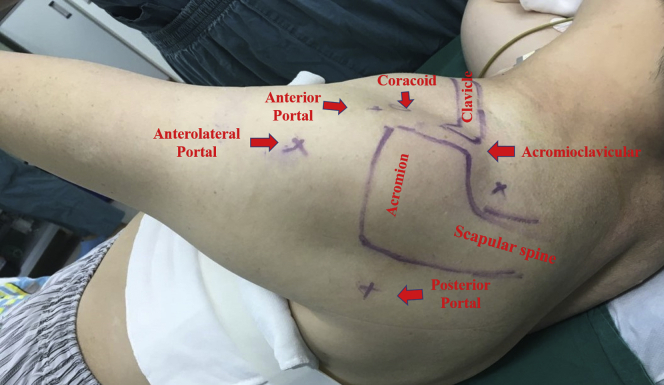
Patient position and landmark identification (left shoulder). The patient is placed in the lateral decubitus position, with continuous affected-extremity traction. The bony landmarks are outlined, and the posterior, anterior, and anterolateral portals are marked.
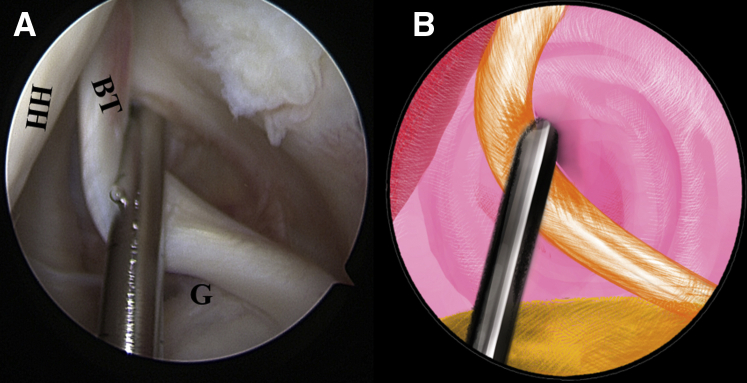
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. A probe from the anterior working portal is used to evaluate the quality of the biceps tendon for an initial assessment. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; G, glenoid; HH, humeral head.).
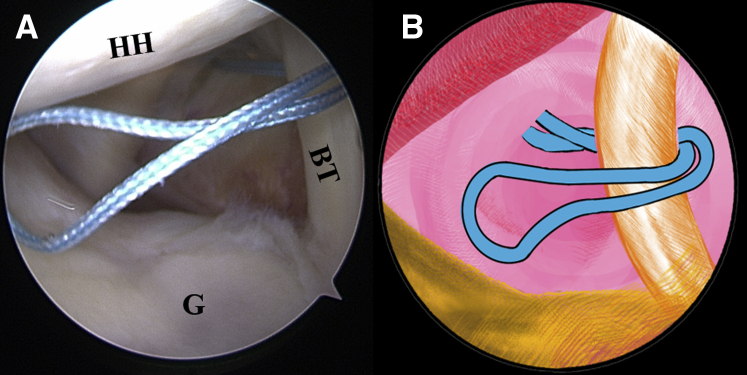
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. A FiberWire is folded in half to be placed at the superior aspect of the biceps tendon through the anterior working portal. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; G, glenoid; HH, humeral head.).
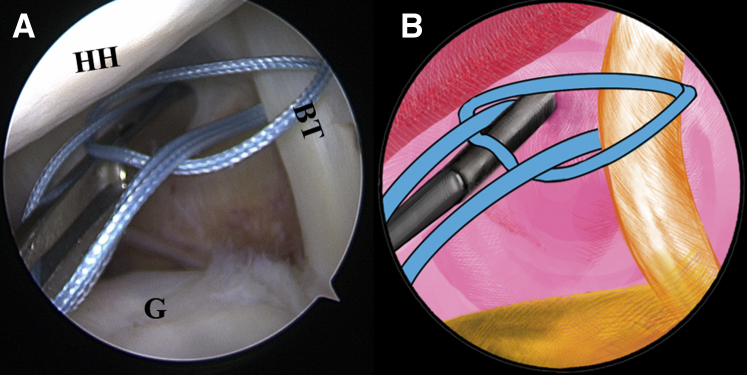
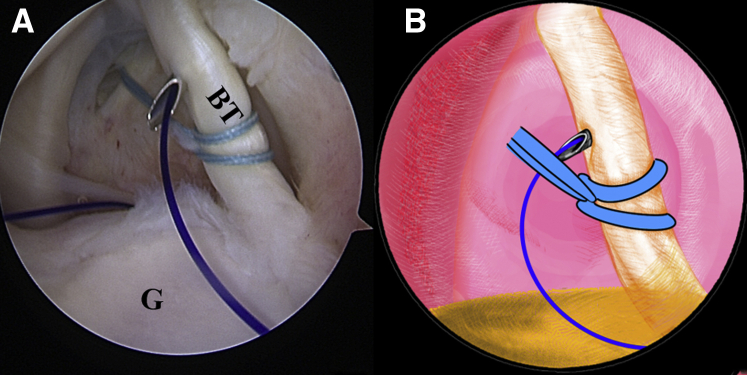
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. Two suture strands are threaded through the loop inferior to the tendon, released, and grasped out of the capsule through the anterior working portal to construct a lark’s head knot. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; G, glenoid; HH, humeral head.).
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. An 18-gauge spinal needle is inserted through the middle portion of the tendon, just distal to the knot, to advance a No. 0 PDS II (polydioxanone) suture. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; G, glenoid.).
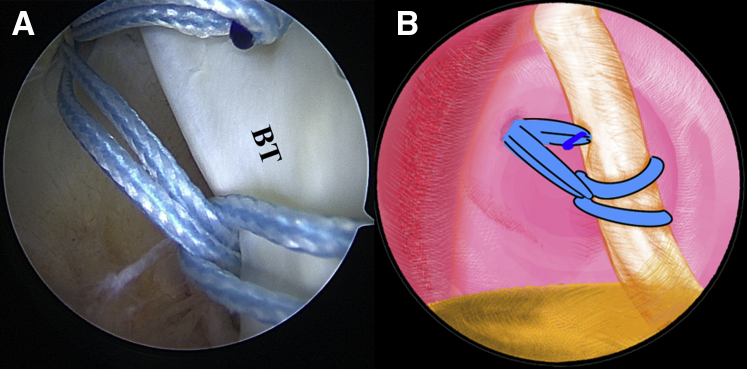
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. An overhand knot has been tied on the 2 strands of the FiberWire ends with the polydioxanone suture. The spinal needle is retrieved, and the polydioxanone suture inside is pulled out, helping to shuttle the 2 strands of FiberWire ends through the tendon. (B) An illustration summarizes the corresponding step. (BT, biceps tendon.).
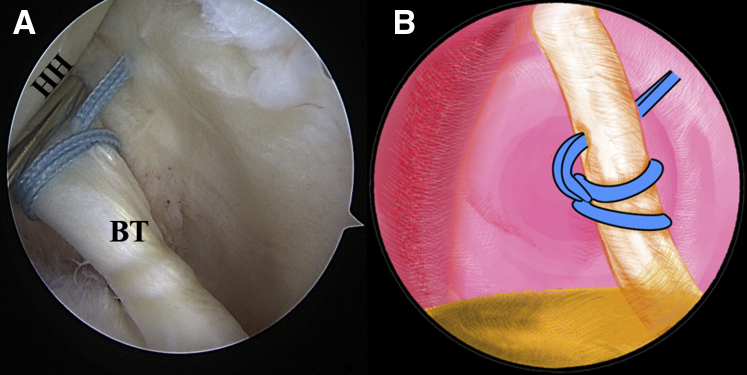
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. Final completion of the lark loop is shown. (B) An illustration summarizes the lark-loop placement on the biceps tendon. (BT, biceps tendon; HH, humeral head.).
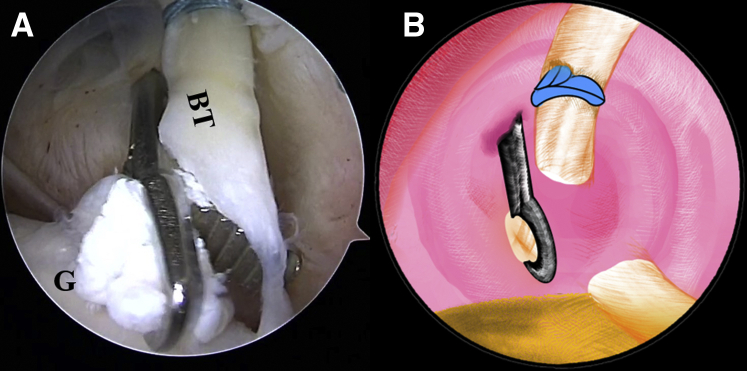
The patient is positioned in the lateral decubitus position. (A) Intra-articular arthroscopic image of a left shoulder from the posterior viewing portal with a 30° arthroscope. The LHBT is detached from its insertion site on the superior-labral junction with a punch forceps through the anterior working portal. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; G, glenoid.).
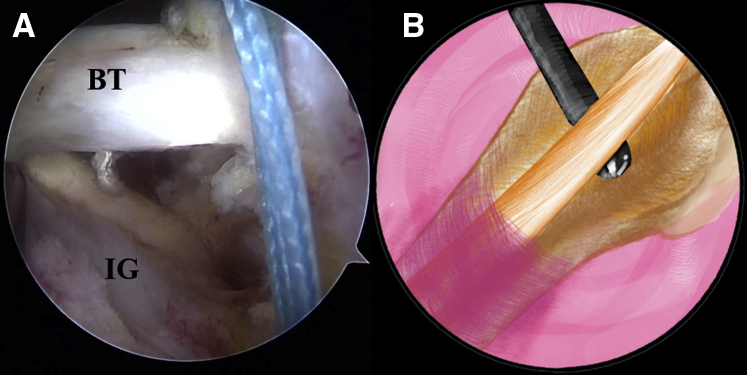
The patient is positioned in the lateral decubitus position. (A) Arthroscopic image in the subacromial space of a left shoulder from the anterolateral viewing portal with a 30° arthroscope. The stump of the biceps tendon is pulled out of the articular cavity. (B) An illustration summarizes the corresponding step. (BT, biceps tendon; IG, intertubercular groove.).
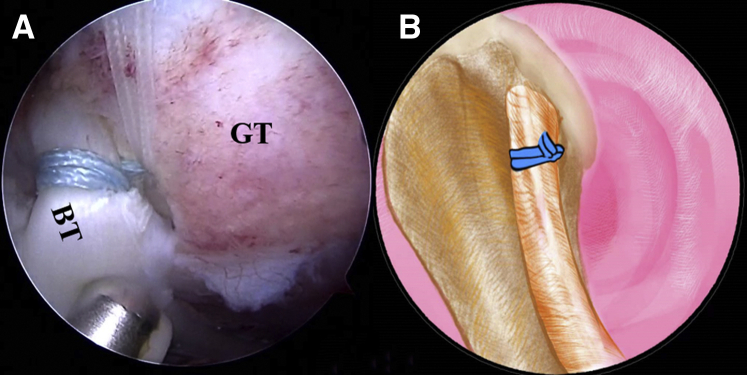
The patient is positioned in the lateral decubitus position. (A) Arthroscopic image in the subacromial space of a left shoulder from the anterolateral viewing portal with a 30° arthroscope. The strands of the lark loop are co-anchored with the lateral row during rotator cuff repair with a 4.75-mm SwiveLock C anchor. (B) An illustration summarizes the strands of the lark loop firmly anchored at the intertubercular groove in the isolated biceps tenodesis with a 4.75-mm SwiveLock C anchor. (BT, biceps tendon; GT, greater tuberosity.).
Similar articles
-
Arthroscopic In Situ Biceps Tenodesis Using a Double Loop-and-Tack Knotless Suture Anchor.Arthrosc Tech. 2023 Jul 31;12(8):e1437-e1442. doi: 10.1016/j.eats.2023.04.014. eCollection 2023 Aug. Arthrosc Tech. 2023. PMID: 37654881 Free PMC article.
-
The "Double Lasso-Loop" Technique Used for Arthroscopic Proximal Biceps Tenodesis.Arthrosc Tech. 2019 Feb 18;8(3):e291-e300. doi: 10.1016/j.eats.2018.11.012. eCollection 2019 Mar. Arthrosc Tech. 2019. PMID: 31016125 Free PMC article.
-
Surgical technique for arthroscopic onlay suprapectoral biceps tenodesis with an all-suture anchor.JSES Open Access. 2018 Mar 13;2(1):69-73. doi: 10.1016/j.jses.2017.12.001. eCollection 2018 Mar. JSES Open Access. 2018. PMID: 30675570 Free PMC article.
-
Suture anchor and percutaneous intra-articular transtendon biceps tenodesis.Sports Med Arthrosc Rev. 2008 Sep;16(3):177-9. doi: 10.1097/JSA.0b013e3181824efd. Sports Med Arthrosc Rev. 2008. PMID: 18703978 Review.
-
Complications of Proximal Biceps Tenotomy and Tenodesis.Clin Sports Med. 2016 Jan;35(1):181-8. doi: 10.1016/j.csm.2015.08.011. Epub 2015 Sep 28. Clin Sports Med. 2016. PMID: 26614476 Review.
Cited by
-
Biomechanical Analysis of Lark-Loop, Lasso-Loop and Krackow Suture Technique in Tenodesis.Orthop Surg. 2023 Apr;15(4):1136-1143. doi: 10.1111/os.13669. Epub 2023 Feb 27. Orthop Surg. 2023. PMID: 36852476 Free PMC article.
References
-
- Khazzam M., George M.S., Churchill R.S., Kuhn J.E. Disorders of the long head of biceps tendon. J Shoulder Elbow Surg. 2012;21:136–145. - PubMed
-
- Elser F., Braun S., Dewing C.B., Giphart J.E., Millett P.J. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. 2011;27:581–592. - PubMed
-
- Patel B.H., Agarwalla A., Lu Y., et al. Isolated biceps tenodesis and tenotomy: A systematic review of indications and patient satisfaction. Orthopedics. 2021;44:333–340. - PubMed
LinkOut - more resources
Full Text Sources
