

Laparoscopic-Assisted Modified Posterior Sagittal Anorectoplasty for Rectobulbar Urethral Fistula of Anorectal Malformation: A Prospective Study
- PMID: 35937122
- PMCID: PMC9350637
- DOI: 10.4103/jiaps.JIAPS_376_20
Laparoscopic-Assisted Modified Posterior Sagittal Anorectoplasty for Rectobulbar Urethral Fistula of Anorectal Malformation: A Prospective Study
Abstract
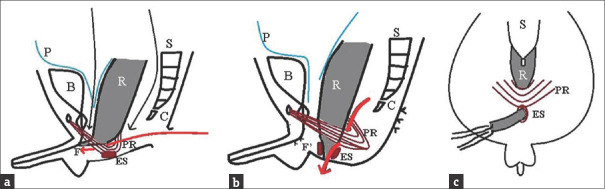
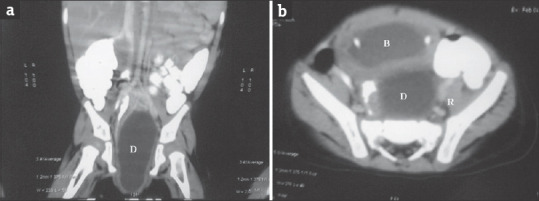
Introduction: Laparoscopic anorectoplasty (LAARP) is useful for the management of rectoprostatic urethral fistula (RPUF), due to easier rectal mobilization, avoidance of posterior sagittal muscular incision, and shorter hospital stay. However, its role in rectobulbar urethral fistula (RBUF) is still debated as there is a chance of urethral diverticulum (UD), due to incomplete dissection. Laparoscopy-assisted modified posterior sagittal anorectoplasty (LAMPSARP) utilizes advantages of LAARP combined with fistula dissection using small sagittal incision preserving puborectalis. The present study compares the results of LAMPSARP with LAARP for correction of RBUF associated with anorectal malformations (ARMs).
Materials and methods: All male ARM with RBUF presenting in a tertiary center in Central India (January 2014-January 2016) were included. Low male ARM, RPUF, rectovesical fistula, and congenital pouch colon were excluded. They were randomized into LAARP and LAMPSARP groups. Complications were assessed in terms of anal stenosis, mucosal prolapse, and UD. Kelly's scoring and Krickenbeck scoring were used to assess continence, and visible anal cosmesis scale (VACS) was used to assess wanal cosmesis. Results were statistically analyzed using a comparison of means and 2 × 2 contingency tables.
Results: Fifty-six colostomized patients with RBUF (26 LAARP, 30 LAMPSARP) were included. Mean operative duration in the LAARP group and LAMPSARP group was 42 ± 10 min and 56 ± 12 min, respectively (P < 0.0001). On mean follow-up of 4.5 years, mucosal prolapse (53.9%) and UD (15.38%) were significantly higher in LAARP group, while anal stenosis was similar. All three, Kelly's score, Krickenbeck score, and VACS, were better (P < 0.05) in the LAMPSARP group.
Conclusion: Laparoscopy-assisted modified posterior sagittal approach is better for RBUF and offers better surgical outcome.
Keywords: Anorectal malformation; laparoscopy; rectobulbar urethral fistula.
Copyright: © 2022 Journal of Indian Association of Pediatric Surgeons.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Georgeson KE, Inge TH, Albanese CT. Laparoscopically assisted anorectal pull-through for high imperforate anus – A new technique. J Pediatr Surg. 2000;35:927–30. - PubMed
-
- Jung SM, Lee SK, Seo JM. Experience with laparoscopic-assisted anorectal pull-through in 25 males with anorectal malformation and rectourethral or rectovesical fistulae: Postoperative complications and functional results. J Pediatr Surg. 2013;48:591–6. - PubMed
-
- López PJ, Guelfand M, Angel L, Paulos A, Cadena Y, Escala JM, et al. Urethral diverticulum after laparoscopically-assisted anorectal pull-through (LAARP) for anorectal malformation: Is resection of the diverticulum always necessary? Arch Esp Urol. 2010;63:297–301. - PubMed
-
- Uchida H, Iwanaka T, Kitano Y, Kudou S, Ishimaru T, Yotsumoto K, et al. Residual fistula after laparoscopically assisted anorectoplasty: Is it a rare problem? J Pediatr Surg. 2009;44:278–81. - PubMed
-
- Liem NT, Quynh TA. Combined laparoscopic and modified posterior sagittal approach saving the external sphincter for rectourethral fistula: An easier and more physiologic approach. J Pediatr Surg. 2013;48:1450–3. - PubMed
LinkOut - more resources
Full Text Sources