

Implementation of Electronic Adherence Monitors and Associated Interventions for Routine HIV Antiretroviral Therapy in Uganda: Promising Findings
- PMID: 35937420
- PMCID: PMC9354256
- DOI: 10.3389/fdgth.2022.899643
Implementation of Electronic Adherence Monitors and Associated Interventions for Routine HIV Antiretroviral Therapy in Uganda: Promising Findings
Abstract
Background: High, sustained adherence is critical for achieving the individual and public health benefits of HIV antiretroviral therapy (ART). Electronic monitors provide detailed adherence information and can enable real-time interventions; however, their use to date has largely been confined to research. This pilot study (NCT03825952) sought to understand feasibility and acceptability a relatively low-cost version of this technology and associated interventions for routine ART delivery in sub-Saharan Africa.
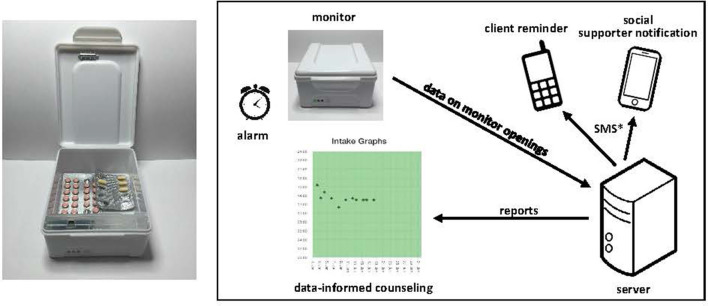
Methods: We provided two ART clinics in rural, southwestern Uganda with electronic adherence monitors for data-informed counseling as well as optional SMS messages to clients and/or social supporters (daily or triggered by missed or delayed doses) and/or an alarm. Clinic and ART client experiences were observed for 3 months per client, including time and motion studies. Qualitative interviews among clients, clinicians, and healthcare administrators were informed by the Consolidated Framework for Implementation Research.
Results: Fifty-one ART clients were enrolled; 57% were male and the median age was 34 years. Choice of associated intervention varied among participants. The median number of visits during follow-up was two per client. Counselors reviewed the adherence data with 90% of clients at least once; 67% reviewed data at all visits. Average adherence was 94%; four clients had adherence gaps >1 week. Acceptability was high; all but one client found the monitor "very useful" and all found SMS "very useful." Clinic visits among clients with the intervention lasted 4 min longer on average than those in standard care. The monitors and daily SMS generally functioned well, although excess SMS were triggered, primarily due to cellular network delays. Overall, participants felt the technology improved adherence, clinic experiences, and clinician-client relationships. Few worried about stigma and privacy. Cost was a concern for implementation, particularly at scale.
Conclusion: We successfully implemented a relatively low-cost electronic ART adherence monitor and associated interventions for routine care in rural Uganda. Feasibility and acceptability were generally high, and individuals were identified who could benefit from adherence support. Future work should involve longitudinal follow-up of diverse populations, clinical outcomes, and detailed cost-effectiveness analysis to help drive policy decisions around the uptake of this technology for routine clinical care.
Clinical trial registration: identifier: NCT03825952.
Keywords: Africa; HIV; SMS intervention; electronic adherence monitoring; implementation science.
Copyright © 2022 Haberer, Baijuka, Tumuhairwe, Tindimwebwa, Tinkamanyire, Tuhanamagyezi, Musoke, Garrison, DelSignore, Musinguzi and Asiimwe.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
Associated data
LinkOut - more resources
Full Text Sources
Medical