

Chronic histiocytic intervillositis (CHI): current treatments and perinatal outcomes, a systematic review and a meta-analysis
- PMID: 35937841
- PMCID: PMC9355722
- DOI: 10.3389/fendo.2022.945543
Chronic histiocytic intervillositis (CHI): current treatments and perinatal outcomes, a systematic review and a meta-analysis
Abstract
Background: Chronic histiocytic intervillositis (CHI) is a rare placental lesion with a high recurrence rate and poor perinatal outcomes. There are currently limited guidelines regarding the diagnosis of this condition in the index pregnancy and treatment where recurrence is suspected.
Objective: The primary objective of this systematic review and meta-analysis was to determine the perinatal outcomes of pregnancies affected by chronic histiocytic intervillositis and to what extent they can be improved with treatment. The secondary objective was to assess the relationship between CHI lesion severity and pregnancy loss.
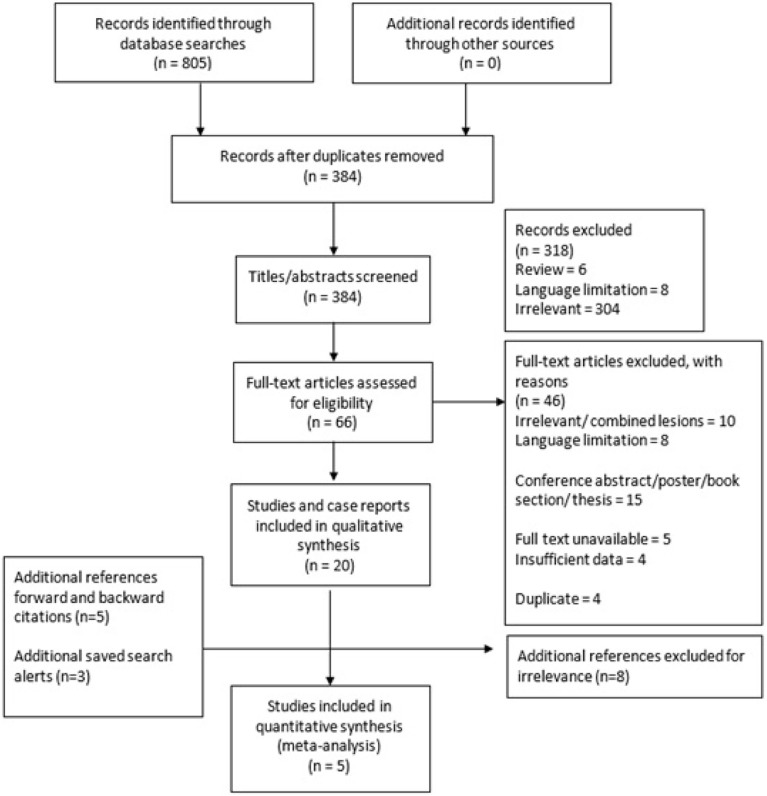
Methods: A systematic search of Ovid Embase, Web of Science, Science Direct, PubMed, Ovid Medline, Google Scholar and CINAHL was carried out. Case reports, cohort, case-control and randomised controlled trials (RCT) detailing the perinatal outcomes of CHI pregnancies, both treated and untreated, were included.
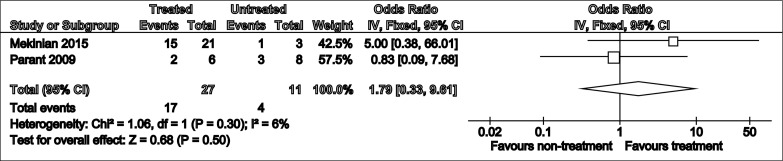
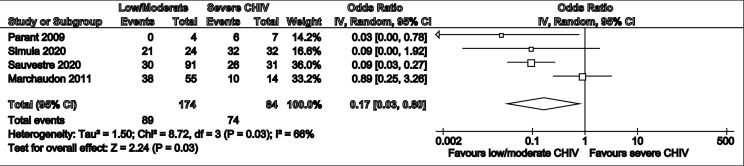
Results: No RCTs were identified. However, in a review population of 659 pregnancies, with additional 7 in case reports, CHI treatments included aspirin, prednisone, prednisolone, low molecular weight heparin (LMWH), hydroxychloroquine and adalimumab. A descriptive synthesis of data found mixed results for treatments in relation to live birth, miscarriage and fetal growth restriction outcomes. Furthermore, quantitative synthesis of 38 pregnancies revealed a non-significant improvement in live birth rate with CHI targeted treatment (OR 1.79 [95% CI 0.33-9.61] (p=0.50), while meta-analysis of CHI severity in line with pregnancy loss, in a sample of 231 pregnancies, revealed lower odds of pregnancy loss with less severe lesions (OR: 0.17 [0.03-0.80], p=0.03).
Conclusions: This systematic review and meta-analysis reinforce notions surrounding the insufficient evidence for CHI treatment. It also strengthens previous hypotheses detailing the positive association between CHI lesion severity and odds of pregnancy loss. Aspirin, LMWH, prednisolone, hydroxychloroquine and adalimumab are candidates with varying levels of weak to moderate evidence supporting their use. Further prospective research is required to obtain robust evidence pertaining to treatment safety and efficacy and optimal drug regimes.
Systematic review registration: [website], identifier CRD42021237604.
Keywords: CHI; intervillositis; recurrent miscarriage; small gestation age (SGA); stillbirth.
Copyright © 2022 Moar, Simela, Nanda, Marnerides, Al-Adnani, Nelson-Piercy, Nicolaides and Shangaris.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Immunomodulatory Therapy Reduces the Severity of Placental Lesions in Chronic Histiocytic Intervillositis.Front Med (Lausanne). 2021 Oct 18;8:753220. doi: 10.3389/fmed.2021.753220. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34733868 Free PMC article.
-
Prevention of recurrent miscarriage in women with antiphospholipid syndrome: A systematic review and network meta-analysis.Lupus. 2021 Jan;30(1):70-79. doi: 10.1177/0961203320967097. Epub 2020 Oct 20. Lupus. 2021. PMID: 33081590
-
Chronic histiocytic intervillositis: outcome, associated diseases and treatment in a multicenter prospective study.Autoimmunity. 2015 Feb;48(1):40-5. doi: 10.3109/08916934.2014.939267. Epub 2014 Jul 16. Autoimmunity. 2015. PMID: 25028066
-
Aspirin or heparin or both for improving pregnancy outcomes in women with persistent antiphospholipid antibodies and recurrent pregnancy loss.Cochrane Database Syst Rev. 2020 May 2;5(5):CD012852. doi: 10.1002/14651858.CD012852.pub2. Cochrane Database Syst Rev. 2020. PMID: 32358837 Free PMC article.
-
Comparison of therapeutic interventions for recurrent pregnancy loss in association with antiphospholipid syndrome: A systematic review and network meta-analysis.Am J Reprod Immunol. 2020 Apr;83(4):e13219. doi: 10.1111/aji.13219. Epub 2020 Jan 28. Am J Reprod Immunol. 2020. PMID: 31872490
Cited by
-
Effect of Anti-TNF Biologic Exposure During Pregnancy on Villitis of Unknown Etiology Diagnoses in Patients with Autoimmune Disease.Reprod Sci. 2024 Apr;31(4):997-1005. doi: 10.1007/s43032-023-01402-w. Epub 2023 Nov 16. Reprod Sci. 2024. PMID: 37973775 Free PMC article.
-
C4d Staining Is Present in Normal Placentas From Pregnancies Prior to Pregnancy Loss Associated With Chronic Histiocytic Intervillositis and Is Reduced by Immunomodulatory Therapy in Subsequent Pregnancies.Pediatr Dev Pathol. 2023 Jul-Aug;26(4):374-387. doi: 10.1177/10935266231176682. Epub 2023 May 26. Pediatr Dev Pathol. 2023. PMID: 37232363 Free PMC article.
-
Virtual crossmatching reveals upregulation of placental HLA-Class II in chronic histiocytic intervillositis.Sci Rep. 2024 Aug 12;14(1):18714. doi: 10.1038/s41598-024-69315-5. Sci Rep. 2024. PMID: 39134702 Free PMC article.
-
Understanding a Potential Role for the NLRP3 Inflammasome in Placenta-Mediated Pregnancy Complications.Am J Reprod Immunol. 2025 Apr;93(4):e70077. doi: 10.1111/aji.70077. Am J Reprod Immunol. 2025. PMID: 40260875 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical