

The incidence of different forms of ileus following surgery for abdominal birth defects in infants: a systematic review with a meta-analysis method
- PMID: 35937853
- PMCID: PMC9294340
- DOI: 10.1515/iss-2020-0042
The incidence of different forms of ileus following surgery for abdominal birth defects in infants: a systematic review with a meta-analysis method
Abstract
Objectives: Ileus following surgery can arise in different forms namely as paralytic ileus, adhesive small bowel obstruction or as anastomotic stenosis. The incidences of these different forms of ileus are not well known after abdominal birth defect surgery in infants. Therefore, this review aims to estimate the incidence in general between abdominal birth defects.
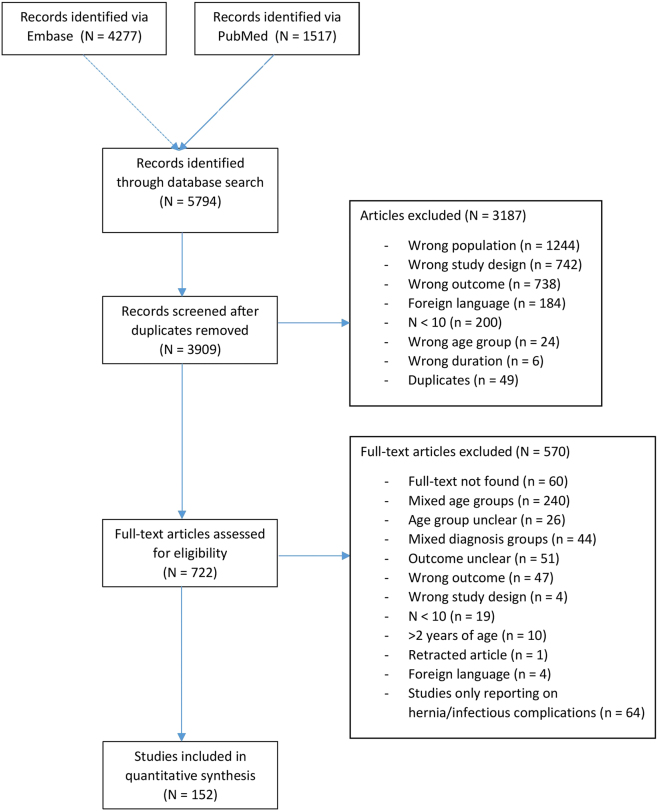
Content: Studies reporting on paralytic ileus, adhesive small bowel obstruction or anastomotic stenosis were considered eligible. PubMed and Embase were searched and risk of bias was assessed. Primary outcome was the incidence of complications. A meta-analysis was performed to pool the reported incidences in total and per birth defect separately.
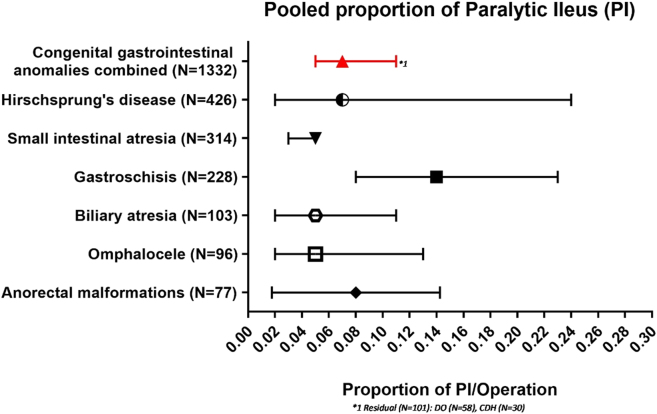
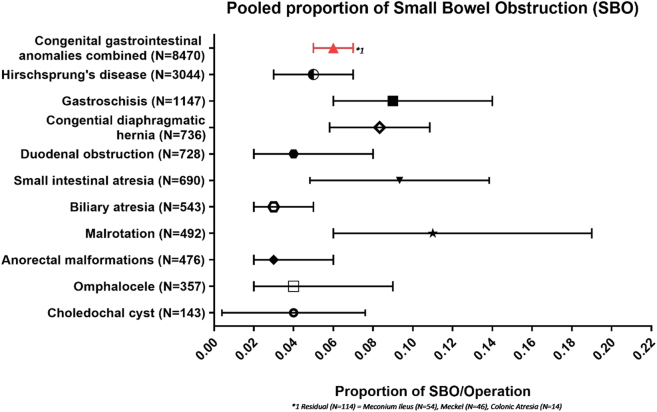
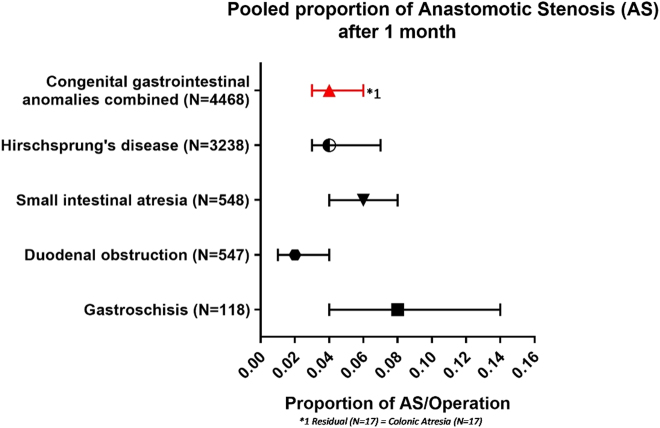
Summary: This study represents a total of 11,617 patients described in 152 studies of which 86 (56%) had a follow-up of at least half a year. Pooled proportions were calculated as follows; paralytic ileus: 0.07 (95%-CI, 0.05-0.11; I 2=71%, p≤0.01) ranging from 0.14 (95% CI: 0.08-0.23) in gastroschisis to 0.05 (95%-CI: 0.02-0.13) in omphalocele. Adhesive small bowel obstruction: 0.06 (95%-CI: 0.05-0.07; I 2=74%, p≤0.01) ranging from 0.11 (95% CI: 0.06-0.19) in malrotation to 0.03 (95% CI: 0.02-0.06) in anorectal malformations. Anastomotic stenosis after a month 0.04 (95%-CI: 0.03-0.06; I 2=59%, p=0.30) ranging from 0.08 (95% CI: 0.04-0.14) in gastroschisis to 0.02 (95% CI: 0.01-0.04) in duodenal obstruction. Anastomotic stenosis within a month 0.03 (95%-CI 0.01-0.10; I 2=81%, p=0.02) was reviewed without separate analysis per birth defect.
Outlook: This review is the first to aggregate the known literature in order approximate the incidence of different forms of ileus for different abdominal birth defects. We showed these complications are common and the distribution varies between birth defects. Knowing which birth defects are most at risk can aid clinicians in taking prompt action, such as nasogastric tube placement, when an ileus is suspected. Future research should focus on the identification of risk factors and preventative measures. The incidences provided by this review can be used in those studies as a starting point for sample size calculations.
Keywords: abdominal birth defect; adhesive small-bowel obstruction; anastomotic stenosis; ileus; infant; paediatric surgery.
© 2021 Laurens D. Eeftinck Schattenkerk et al., published by De Gruyter, Berlin/Boston.
Conflict of interest statement
Competing interests: Authors state no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources