

Simultaneous measurement of diaphragm activity, chest impedance, and ECG using three standard cardiorespiratory monitoring electrodes
- PMID: 35938231
- PMCID: PMC9804169
- DOI: 10.1002/ppul.26096
Simultaneous measurement of diaphragm activity, chest impedance, and ECG using three standard cardiorespiratory monitoring electrodes
Abstract
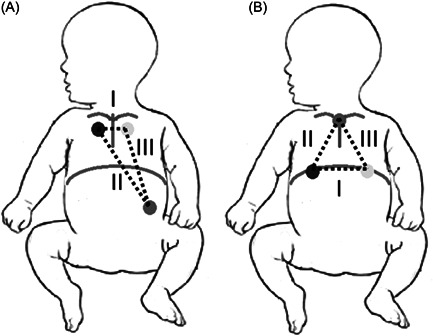
Introduction: Current cardiorespiratory monitoring in neonates with electrocardiogram (ECG) and chest impedance (CI) has limitations. Adding transcutaneous electromyography of the diaphragm (dEMG) may improve respiratory monitoring, but requires additional hardware. We aimed to determine the feasibility of measuring dEMG and ECG/CI simultaneously using the standard ECG/CI hardware, with its three electrodes repositioned to dEMG electrode locations.
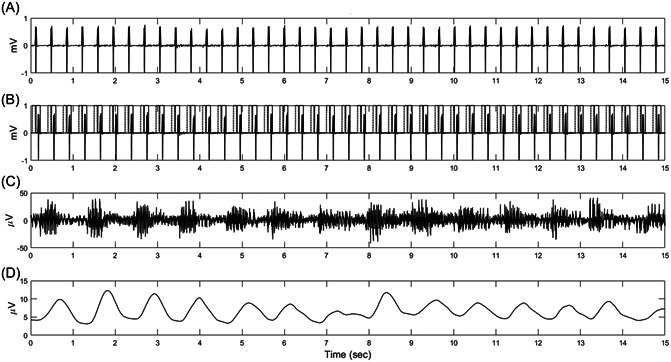
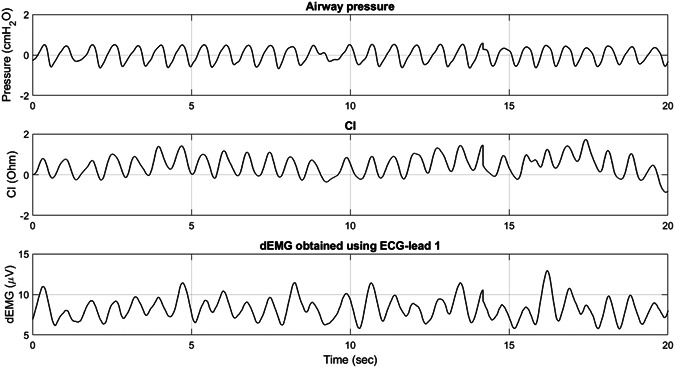
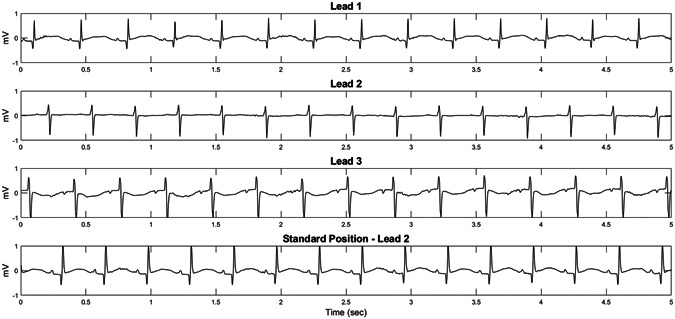
Methods: Thirty infants (median postmenstrual age 30.4 weeks) were included. First, we assessed the feasibility of extracting dEMG from the ECG-signal. If successful, the agreement between dEMG-based respiratory rate (RR), using three different ECG-leads, and a respiratory reference signal was assessed using the Bland-Altman analysis and the intraclass correlation coefficient (ICC). Furthermore, we studied the agreement between CI-based RR and the reference signal with the electrodes placed at the standard and dEMG position. Finally, we explored the quality of the ECG-signal at the different electrode positions.
Results: In 15 infants, feasibility of measuring dEMG with the monitoring electrodes was confirmed. In the next 15 infants, comparing dEMG-based RR to the reference signal resulted in a mean difference and limits of agreement for ECG-lead I, II and III of 4.2 [-8.2 to 16.6], 4.3 [-10.7 to 19.3] and 5.0 [-14.2 to 24.2] breaths/min, respectively. ICC analysis showed a moderate agreement for all ECG-leads. CI-based RR agreement was similar at the standard and dEMG electrode position. An exploratory analysis suggested similar quality of the ECG-signal at both electrode positions.
Conclusion: Measuring dEMG using the ECG/CI hardware with its electrodes on the diaphragm is feasible, leaving ECG/CI monitoring unaffected.
Keywords: neonates; respiration; transcutaneous electromyography.
© 2022 The Authors. Pediatric Pulmonology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Cardiorespiratory monitoring in the delivery room using transcutaneous electromyography.Arch Dis Child Fetal Neonatal Ed. 2021 Jul;106(4):352-356. doi: 10.1136/archdischild-2020-319535. Epub 2020 Nov 19. Arch Dis Child Fetal Neonatal Ed. 2021. PMID: 33214154
-
Transcutaneous electromyography of the diaphragm: A cardio-respiratory monitor for preterm infants.Pediatr Pulmonol. 2015 Sep;50(9):889-95. doi: 10.1002/ppul.23116. Epub 2014 Oct 18. Pediatr Pulmonol. 2015. PMID: 25327880
-
Diaphragmatic electromyography in preterm infants: The influence of electrode positioning.Pediatr Pulmonol. 2020 Feb;55(2):354-359. doi: 10.1002/ppul.24585. Epub 2019 Nov 25. Pediatr Pulmonol. 2020. PMID: 31765520 Free PMC article.
-
Development of three methods for extracting respiration from the surface ECG: a review.J Electrocardiol. 2014 Nov-Dec;47(6):819-25. doi: 10.1016/j.jelectrocard.2014.07.020. Epub 2014 Aug 4. J Electrocardiol. 2014. PMID: 25194875 Review.
-
Diaphragmatic electromyography in infants: an overview of possible clinical applications.Pediatr Res. 2024 Jan;95(1):52-58. doi: 10.1038/s41390-023-02800-1. Epub 2023 Sep 2. Pediatr Res. 2024. PMID: 37660179 Review.
References
-
- Di Fiore JM, Poets CF, Gauda E, Martin RJ, MacFarlane P. Cardiorespiratory events in preterm infants: etiology and monitoring technologies. J Perinatol. 2016;36(3):165‐171. - PubMed
-
- Poets CF, Roberts RS, Schmidt B, et al. Association between intermittent hypoxemia or bradycardia and late death or disability in extremely preterm infants. JAMA. 2015;314(6):595‐603. - PubMed
-
- Di Fiore JM. Neonatal cardiorespiratory monitoring techniques. Semin Neonatol. 2004;9(3):195‐203. - PubMed
-
- Kraaijenga JV, Hutten GJ, de Jongh FH, van Kaam AH. Transcutaneous electromyography of the diaphragm: a cardio‐respiratory monitor for preterm infants. Pediatr Pulmonol. 2015;50(9):889‐895. - PubMed
-
- Kraaijenga JV, de Waal CG, Hutten GJ, de Jongh FH, van Kaam AH. Diaphragmatic activity during weaning from respiratory support in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2017;102(4):F307‐F311. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
