

Serious adverse event rates and reoperation after arthroscopic shoulder surgery: population based cohort study
- PMID: 35938625
- PMCID: PMC9258605
- DOI: 10.1136/bmj-2021-069901
Serious adverse event rates and reoperation after arthroscopic shoulder surgery: population based cohort study
Abstract
Objective: To provide clinicians and patients with accurate risk estimates of serious adverse events after common elective shoulder arthroscopic procedures, including reoperation within one year.
Design: Population based cohort study.
Setting: Hospital Episode Statistics for NHS England, including civil registration mortality data from the Office for National Statistics.
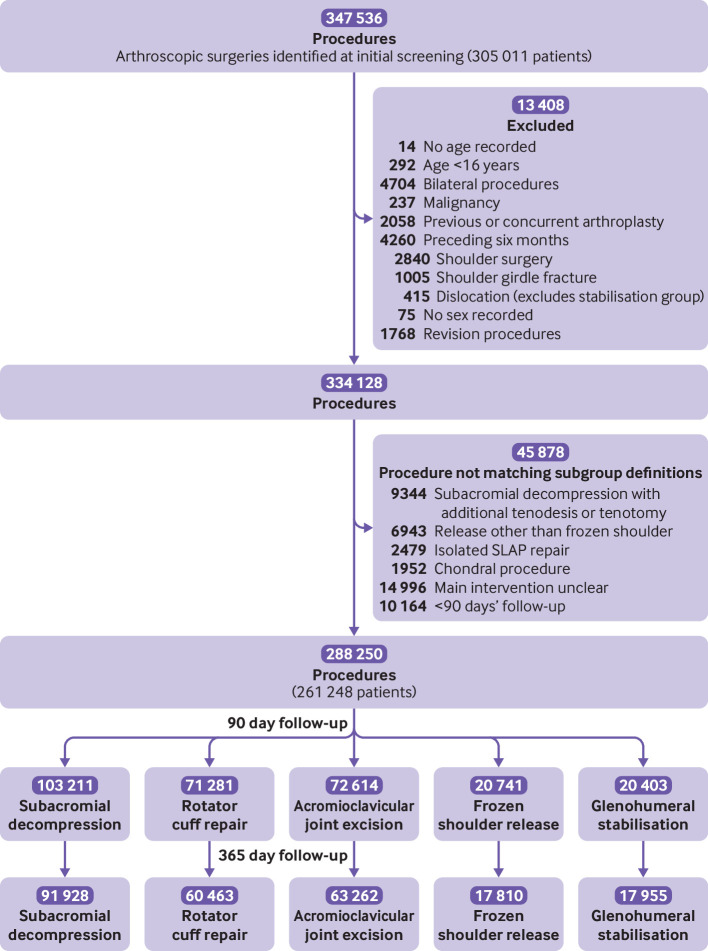
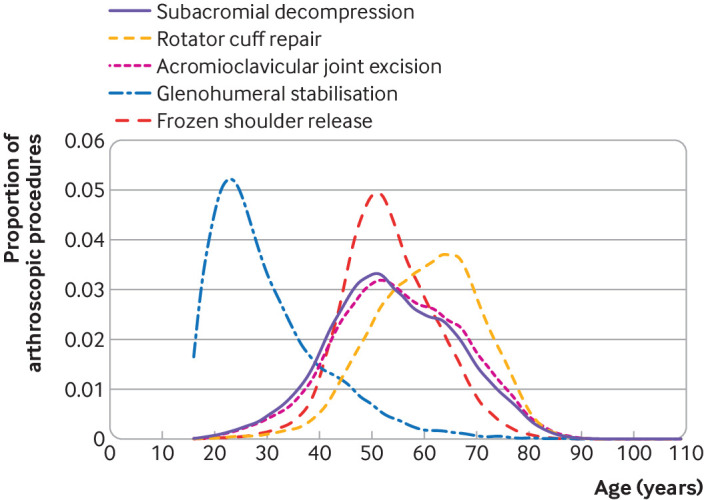
Participants: 288 250 arthroscopic shoulder procedures performed in 261 248 patients aged ≥16 years between 1 April 2009 and 31 March 2017. Elective procedures were grouped into subacromial decompression, rotator cuff repair, acromioclavicular joint excision, glenohumeral stabilisation, and frozen shoulder release.
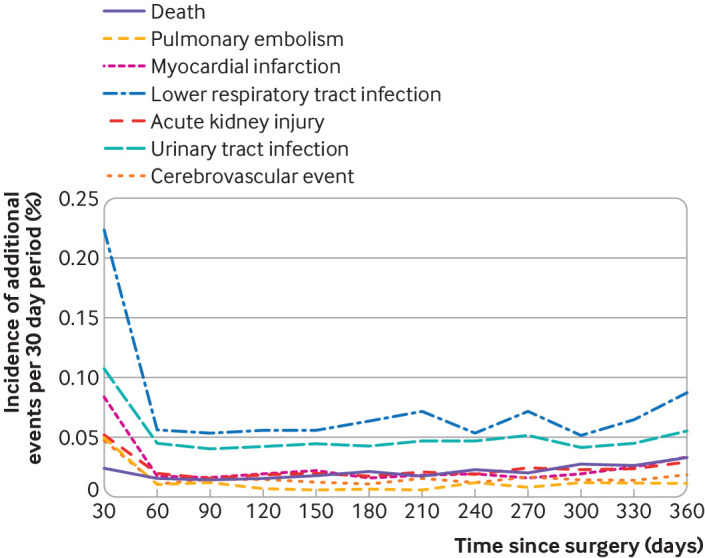
Main outcome measures: The primary outcomes were rates of serious adverse events (mortality, pulmonary embolism, pneumonia, myocardial infarction, acute kidney injury, stroke, and urinary tract infection) requiring inpatient care within 90 days post-surgery. Secondary outcomes were specific adverse event rates at 90 days, and reoperations (including for deep infection) within one year.
Results: The overall rate of complications within 90 days after arthroscopic shoulder surgery (including reoperation) was low at 1.2% (95% confidence interval 1.2% to 1.3%), with one in 81 patients at risk, and varied according to type of procedure, from 0.6% (0.5% to 0.8%) for glenohumeral stabilisation to 1.7% (1.5% to 1.8%) for frozen shoulder release. After adjustment for age, comorbidities, and sex, no effect of procedure type was observed. Pneumonia was the most common adverse event (0.3%, 0.3% to 0.4%), with one in 303 patients at risk. Pulmonary embolic events were rare, at 0.1% (0.1% to 0.1%), with one in 1428 patients at risk. At one year, the overall rate for reoperation was 3.8% (3.8% to 3.9%), with one in 26 patients at risk, ranging from 2.7% (2.5% to 3.0%) for glenohumeral stabilisation to 5.7% (5.4% to 6.1%) for frozen shoulder release. The overall rate of further surgery for deep infection was low, at 0.1% (0.1% to 0.1%), with one in 1111 patients at risk, but was higher after rotator cuff repair (0.2%, 0.2% to 0.2%), with one in 526 patients at risk. Over the study period the number of arthroscopic shoulder procedures increased, except for subacromial decompression, which decreased.
Conclusions: The findings of this study suggest that risks of serious adverse events associated with common shoulder arthroscopy procedures are low. Nevertheless, serious complications do occur, and include the risk of reoperation in one in 26 patients within one year.
Study registration: Clinical.
Trials: gov NCT03573765.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; JCEL reports grants from Versus Arthritis, grants from Medical Research Council, outside the submitted work. DPA reports grants from Amgen for speaker services and advisory board membership, consultancy fees from UCB Biopharma and Astra Zeneca, and grants from European Medicines Agency and UCB Biopharma all outside the submitted work. DPA also reports support for training programmes from Janssen, on behalf of Innovative Medicines Initiative (IMI)-funded European Health Data and Evidence Network, and Synapse Management Partners. These programmes run by DPA are open to external participants. AJC reports grants from the National Institute for Health and Care Research and grants from the Wellcome Trust during the conduct of the study; in addition, AJC has a patent BioPatch issued and sits on Novartis Musculoskeletal advisory board and UKRI Advanced Pain Discovery programme; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Serious adverse events and lifetime risk of reoperation after elective shoulder replacement: population based cohort study using hospital episode statistics for England.BMJ. 2019 Feb 20;364:l298. doi: 10.1136/bmj.l298. BMJ. 2019. PMID: 30786996 Free PMC article.
-
Incidence of acute postoperative infections requiring reoperation after arthroscopic shoulder surgery.Am J Sports Med. 2014 Feb;42(2):437-41. doi: 10.1177/0363546513510686. Epub 2013 Dec 2. Am J Sports Med. 2014. PMID: 24296963
-
Does Distal Clavicle Resection Decrease Pain or Improve Shoulder Function in Patients With Acromioclavicular Joint Arthritis and Rotator Cuff Tears? A Meta-analysis.Clin Orthop Relat Res. 2018 Dec;476(12):2402-2414. doi: 10.1097/CORR.0000000000000424. Clin Orthop Relat Res. 2018. PMID: 30334833 Free PMC article.
-
Reverse total shoulder replacement versus anatomical total shoulder replacement for osteoarthritis: population based cohort study using data from the National Joint Registry and Hospital Episode Statistics for England.BMJ. 2024 Apr 30;385:e077939. doi: 10.1136/bmj-2023-077939. BMJ. 2024. PMID: 38688550 Free PMC article.
-
[Differential therapy for the rheumatoid shoulder].Orthopade. 2002 Dec;31(12):1132-44. doi: 10.1007/s00132-002-0401-2. Orthopade. 2002. PMID: 12486539 Review. German.
Cited by
-
Percutaneous bone marrow concentrate and platelet products versus exercise therapy for the treatment of rotator cuff tears: a randomized controlled, crossover trial with 2-year follow-up.BMC Musculoskelet Disord. 2024 May 18;25(1):392. doi: 10.1186/s12891-024-07519-6. BMC Musculoskelet Disord. 2024. PMID: 38762734 Free PMC article. Clinical Trial.
-
Pediatric Shoulder Arthroscopy is Effective and Most Commonly Indicated for Instability, Obstetric Brachial Plexus Palsy, and Partial Rotator Cuff Tears.Arthrosc Sports Med Rehabil. 2023 Jan 2;5(1):e281-e295. doi: 10.1016/j.asmr.2022.11.016. eCollection 2023 Feb. Arthrosc Sports Med Rehabil. 2023. PMID: 36866288 Free PMC article. Review.
-
Pulmonary embolism after shoulder surgery: Is it a real threat?World J Methodol. 2025 Mar 20;15(1):98343. doi: 10.5662/wjm.v15.i1.98343. eCollection 2025 Mar 20. World J Methodol. 2025. PMID: 40115404 Free PMC article. Review.
-
The effects of telemedicine on Rotator cuff-related shoulder function and pain symptoms: a meta-analysis of randomized clinical trials.J Orthop Surg Res. 2024 Aug 14;19(1):478. doi: 10.1186/s13018-024-04986-4. J Orthop Surg Res. 2024. PMID: 39143625 Free PMC article.
-
Resorbable Bio-Inductive Collagen Implant for Rotator Cuff Repair: What We Know, What We Need to Know, and the Path Forward.Orthop Surg. 2025 Sep;17(9):2541-2557. doi: 10.1111/os.70141. Epub 2025 Aug 8. Orthop Surg. 2025. PMID: 40781789 Free PMC article. Review.
References
-
- GBD 2017 . Disease and Injury Incidence and Prevalence Collaborators SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392:1789-858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
-
- Abram SGF, Judge A, Beard DJ, Wilson HA, Price AJ. Temporal trends and regional variation in the rate of arthroscopic knee surgery in England: analysis of over 1.7 million procedures between 1997 and 2017. Has practice changed in response to new evidence? Br J Sports Med 2019;53:1533-8. 10.1136/bjsports-2018-099414. - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous