

Malnutrition and immune cell subsets in children undergoing kidney transplantation
- PMID: 35938682
- PMCID: PMC9669171
- DOI: 10.1111/petr.14371
Malnutrition and immune cell subsets in children undergoing kidney transplantation
Abstract
Background: Malnutrition, including obesity and undernutrition, among children is increasing in prevalence and is common among children on renal replacement therapy. The effect of malnutrition on the pre-transplant immune system and how the pediatric immune system responds to the insult of both immunosuppression and allotransplantation is unknown. We examined the relationship of nutritional status with post-transplant outcomes and characterized the peripheral immune cell phenotypes of children from the Immune Development of Pediatric Transplant (IMPACT) study.
Methods: Ninety-eight patients from the IMPACT study were classified as having obesity, undernutrition, or normal nutrition-based pre-transplant measurements. Incidence of infectious and alloimmune outcomes at 1-year post-transplantation was compared between nutritional groups using Gray's test and Fine-Gray subdistribution hazards model. Event-free survival was estimated by Kaplan-Meier method and compared between groups. Differences in immune cell subsets between nutritional groups over time were determined using generalized estimating equations accounting for the correlation between repeated measurements.
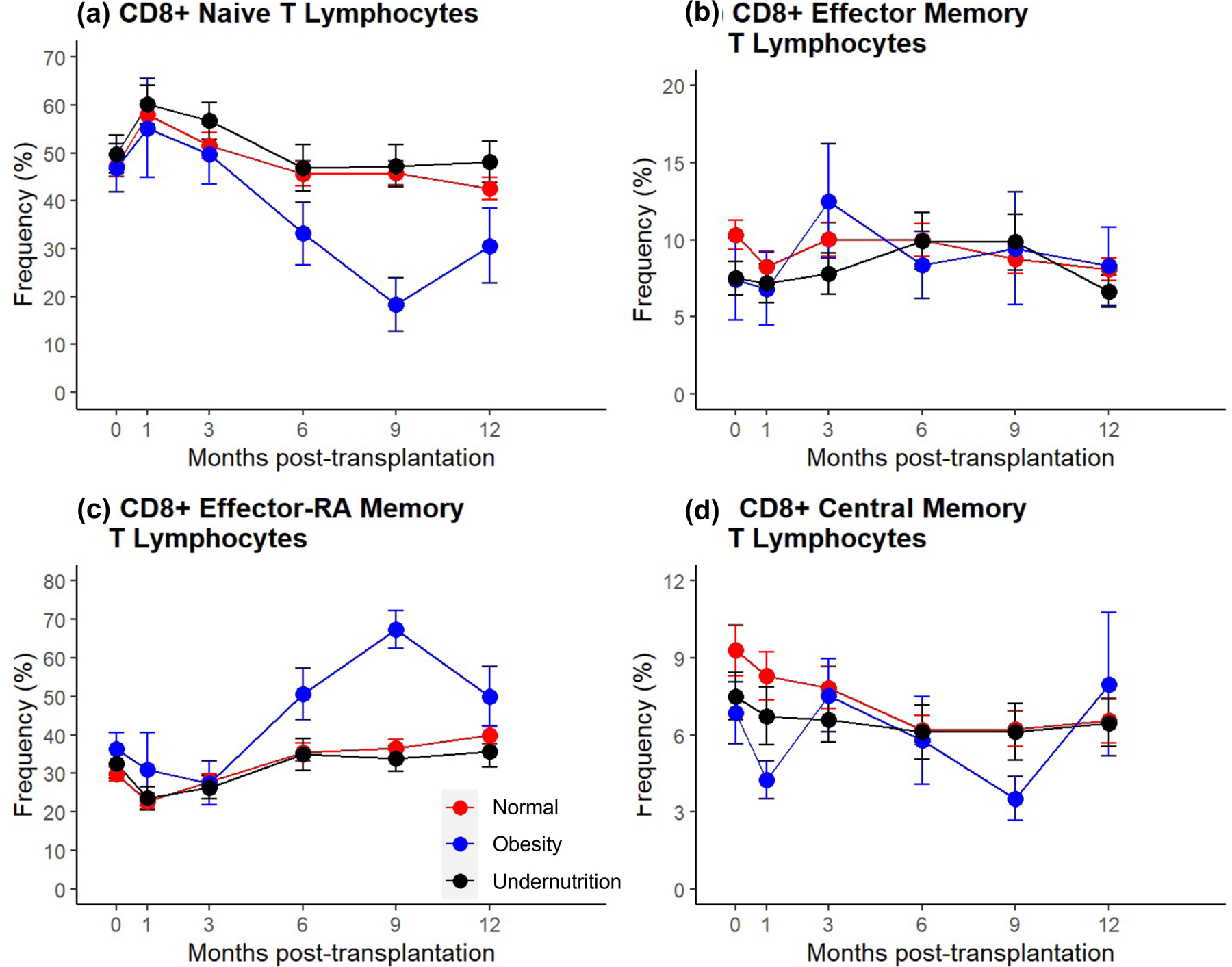
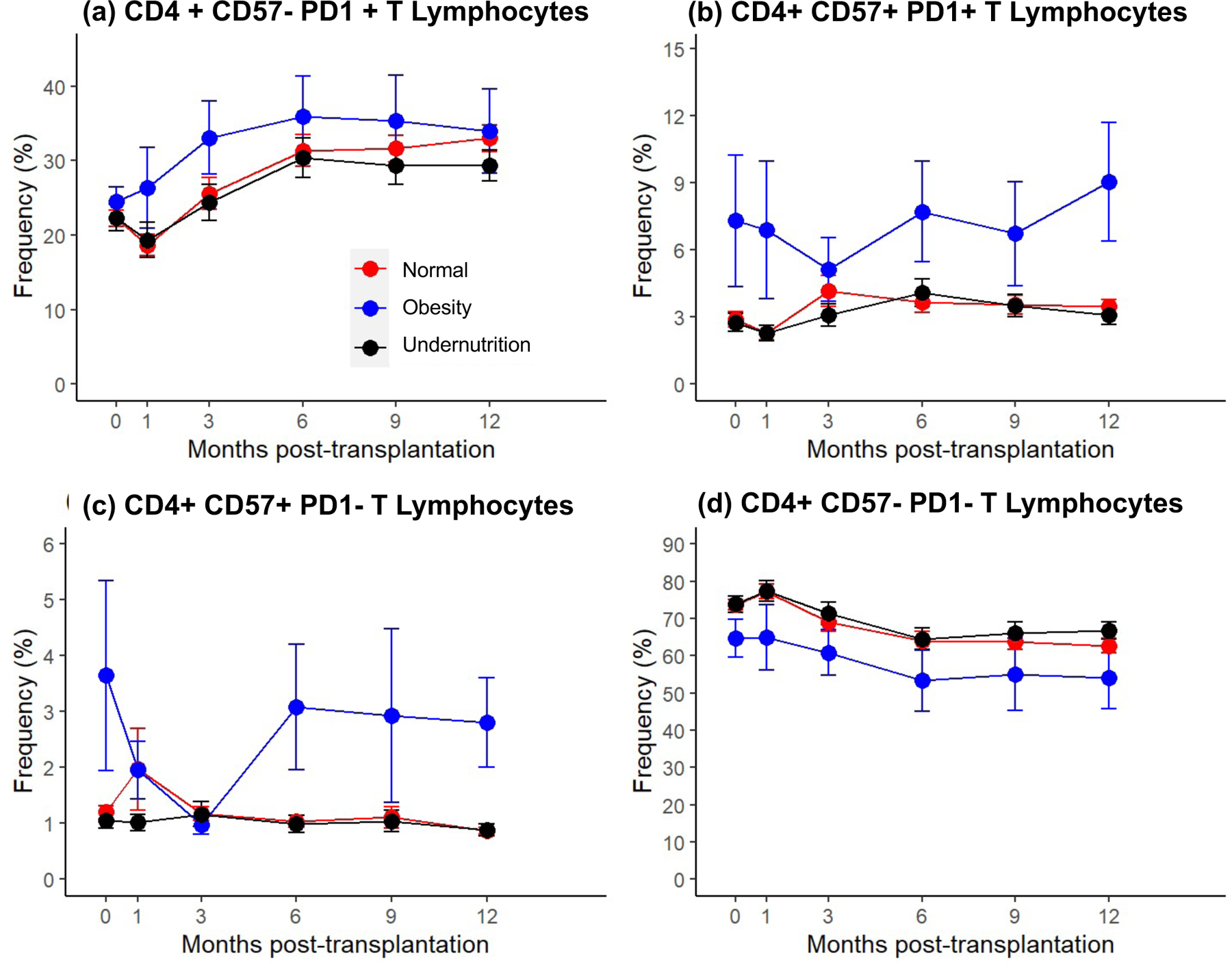
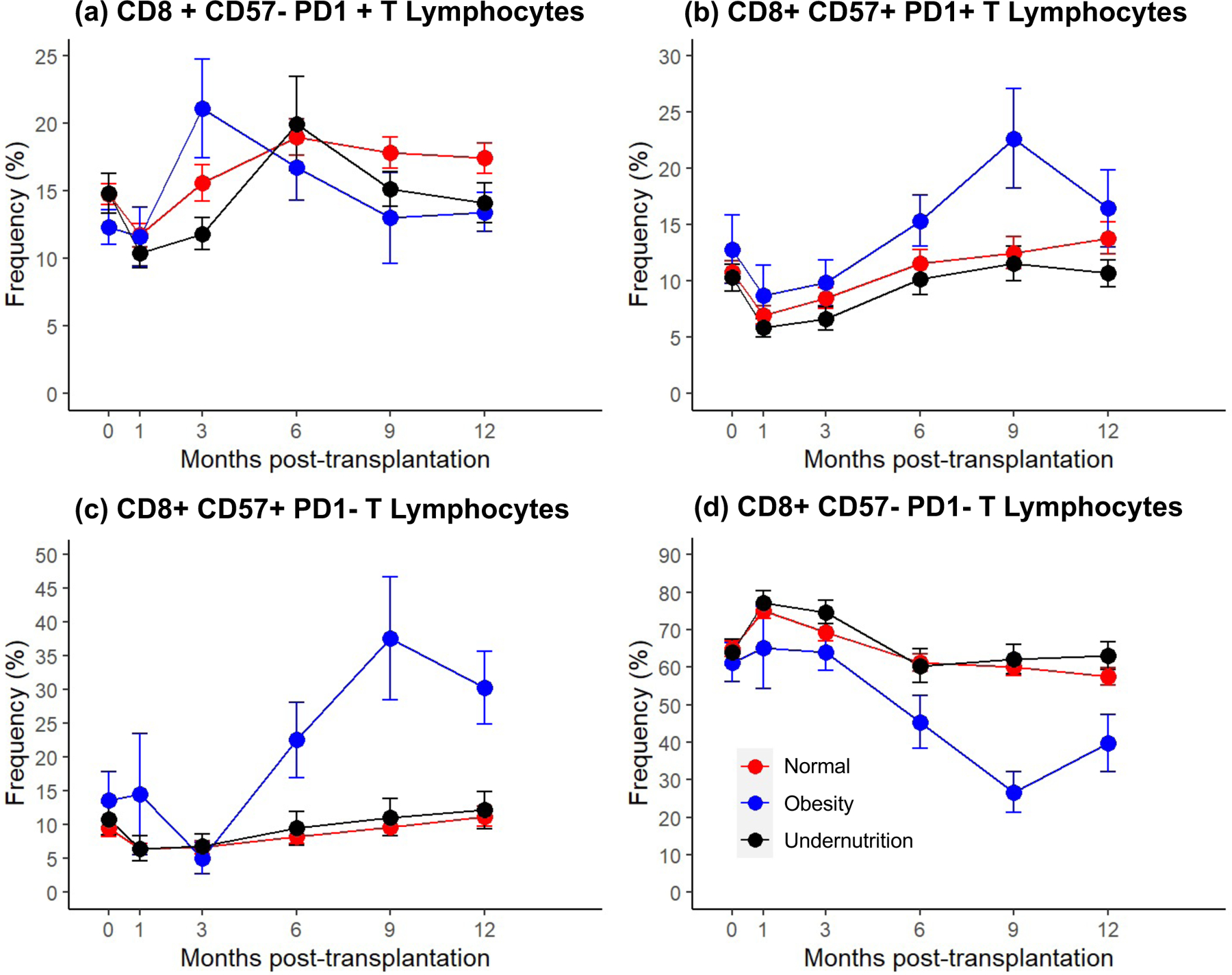
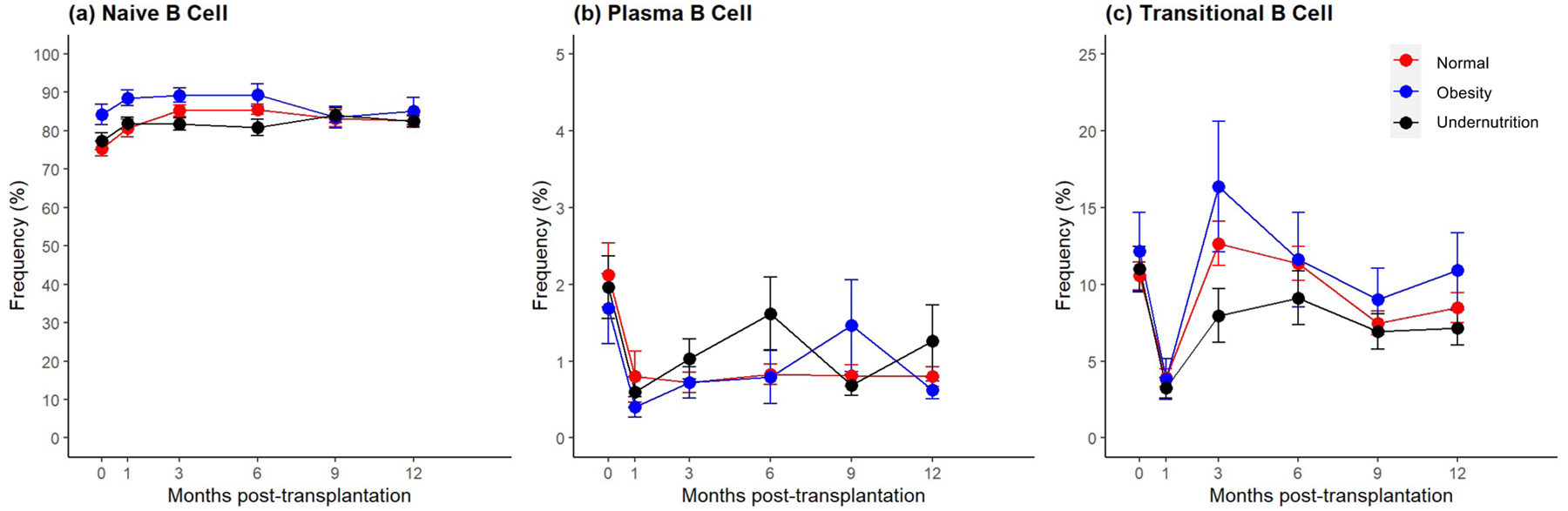
Results: We did not observe that nutritional status was associated with infectious or alloimmune events or event-free survival post-transplant. We demonstrated that children with obesity had distinct T-and B-cell signatures relative to those with undernutrition and normal nutrition, even when controlling for immunosuppression. Children with obesity had a lower frequency of CD8 Tnaive cells 9-month post-transplant (p < .001), a higher frequency of CD4 CD57 + PD1- T cells, and lower frequencies of CD57-PD1+ CD8 and CD57-PD1- CD8 T cells at 12-month transplant (p < .05 for all).
Conclusions: Children with obesity have distinct immunophenotypes that may influence the tailoring of immunosuppression.
Keywords: immunosuppression; immunosuppressive treatment; induction; kidney.
© 2022 Wiley Periodicals LLC.
Conflict of interest statement
Disclosures
The authors of this manuscript have no conflicts of interest to disclose.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
