

Patient-Centered Pain Care Using Artificial Intelligence and Mobile Health Tools: A Randomized Comparative Effectiveness Trial
- PMID: 35939288
- PMCID: PMC9361183
- DOI: 10.1001/jamainternmed.2022.3178
Patient-Centered Pain Care Using Artificial Intelligence and Mobile Health Tools: A Randomized Comparative Effectiveness Trial
Abstract
Importance: Cognitive behavioral therapy for chronic pain (CBT-CP) is a safe and effective alternative to opioid analgesics. Because CBT-CP requires multiple sessions and therapists are scarce, many patients have limited access or fail to complete treatment.
Objectives: To determine if a CBT-CP program that personalizes patient treatment using reinforcement learning, a field of artificial intelligence (AI), and interactive voice response (IVR) calls is noninferior to standard telephone CBT-CP and saves therapist time.
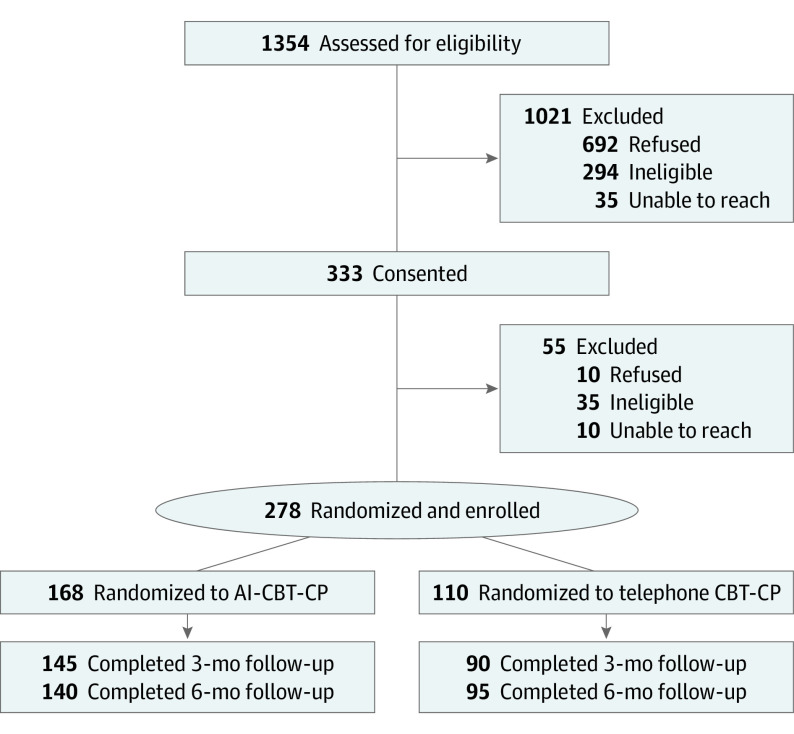
Design, setting, and participants: This was a randomized noninferiority, comparative effectiveness trial including 278 patients with chronic back pain from the Department of Veterans Affairs health system (recruitment and data collection from July 11, 2017-April 9, 2020). More patients were randomized to the AI-CBT-CP group than to the control (1.4:1) to maximize the system's ability to learn from patient interactions.
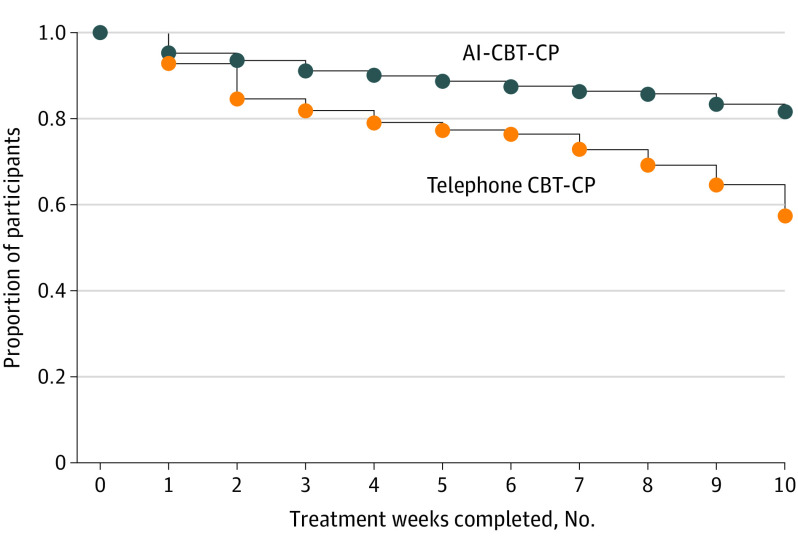
Interventions: All patients received 10 weeks of CBT-CP. For the AI-CBT-CP group, patient feedback via daily IVR calls was used by the AI engine to make weekly recommendations for either a 45-minute or 15-minute therapist-delivered telephone session or an individualized IVR-delivered therapist message. Patients in the comparison group were offered 10 therapist-delivered telephone CBT-CP sessions (45 minutes/session).
Main outcomes and measures: The primary outcome was the Roland Morris Disability Questionnaire (RMDQ; range 0-24), measured at 3 months (primary end point) and 6 months. Secondary outcomes included pain intensity and pain interference. Consensus guidelines were used to identify clinically meaningful improvements for responder analyses (eg, a 30% improvement in RMDQ scores and pain intensity). Data analyses were performed from April 2021 to May 2022.
Results: The study population included 278 patients (mean [SD] age, 63.9 [12.2] years; 248 [89.2%] men; 225 [81.8%] White individuals). The 3-month mean RMDQ score difference between AI-CBT-CP and standard CBT-CP was -0.72 points (95% CI, -2.06 to 0.62) and the 6-month difference was -1.24 (95% CI, -2.48 to 0); noninferiority criterion were met at both the 3- and 6-month end points (P < .001 for both). A greater proportion of patients receiving AI-CBT-CP had clinically meaningful improvements at 6 months as indicated by RMDQ (37% vs 19%; P = .01) and pain intensity scores (29% vs 17%; P = .03). There were no significant differences in secondary outcomes. Pain therapy using AI-CBT-CP required less than half of the therapist time as standard CBT-CP.
Conclusions and relevance: The findings of this randomized comparative effectiveness trial indicated that AI-CBT-CP was noninferior to therapist-delivered telephone CBT-CP and required substantially less therapist time. Interventions like AI-CBT-CP could allow many more patients to be served effectively by CBT-CP programs using the same number of therapists.
Trial registration: ClinicalTrials.gov Identifier: NCT02464449.
Conflict of interest statement
Figures
References
-
- Croft P, Blyth FM, van der Windt D. Chronic pain as a topic for epidemiology and public health. In: Croft P, Blyth FM, van der Windt D, eds. Chronic Pain Epidemiology: From Etiology to Public Health. Oxford; 2011:3-8.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
