

Prevalence and outcomes of patients developing heparin-induced thrombocytopenia during extracorporeal membrane oxygenation
- PMID: 35939484
- PMCID: PMC9359525
- DOI: 10.1371/journal.pone.0272577
Prevalence and outcomes of patients developing heparin-induced thrombocytopenia during extracorporeal membrane oxygenation
Abstract
Objectives: Unfractionated heparin (UFH) is the commonly used anticoagulant to prevent clotting of the ECMO circuit and thrombosis of the cannulated vessels. A side effect of UFH is heparin-induced thrombocytopenia (HIT). Little is known about HIT during ECMO and the impact of changing anticoagulation in ECMO patients with newly diagnosed HIT. The aim of the study was to determine the prevalence, complications, impact of switching anticoagulation to argatroban and outcomes of patients developing heparin-induced thrombocytopenia (HIT) during either veno-venous (VV) or veno-arterial (VA) ECMO.
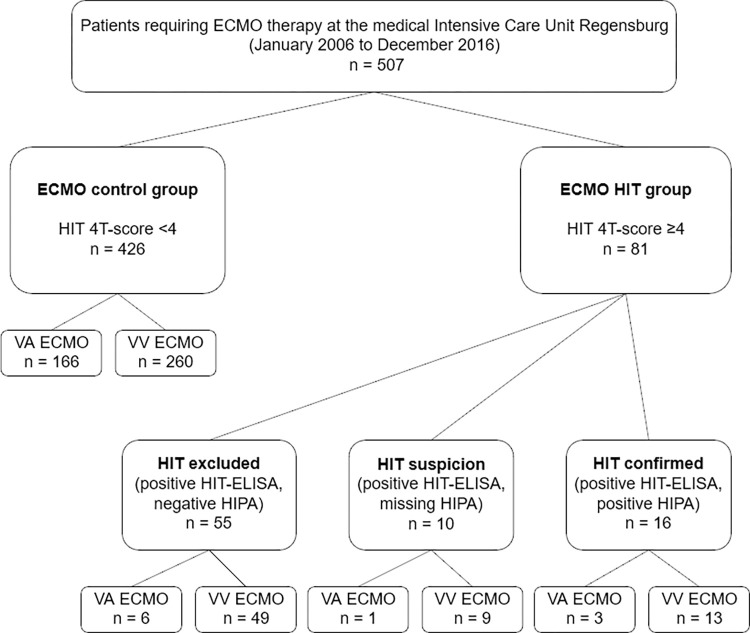
Methods: Retrospective observational single centre study of prospectively collected data of consecutive patients receiving VV ECMO therapy for severe respiratory failure and VA ECMO for circulatory failure from January 2006 to December 2016 of the Medical intensive care unit (ICU) of the University Hospital of Regensburg. Treatment of HIT on ECMO was done with argatroban.
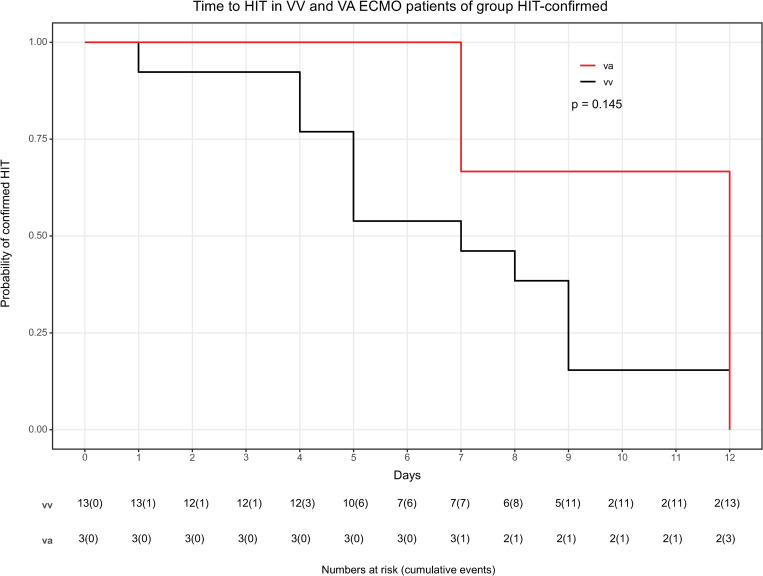
Results: 507 patients requiring ECMO were included. Further HIT-diagnostic was conducted if HIT-4T-score was ≥4. The HIT-confirmed group had positive HIT-enzyme-linked-immunosorbent-assay (ELISA) and positive heparin-induced-platelet-activation (HIPA) test, the HIT-suspicion group a positive HIT-ELISA and missing HIPA but remained on alternative anticoagulation until discharge and the HIT-excluded group a negative or positive HIT-ELISA, however negative HIPA. These were compared to group ECMO-control without any HIT suspicion. The prevalence of HIT-confirmed was 3.2%, of HIT-suspicion 2.0% and HIT-excluded 10.8%. Confirmed HIT was trendwise more frequent in VV than in VA (3.9 vs. 1.7% p = 0.173). Compared to the ECMO control group, patients with confirmed HIT were longer on ECMO (median 13 vs. 8 days, p = 0.002). Different types of complications were higher in the HIT-confirmed than in the ECMO-control group, but in-hospital mortality was not different (31% vs. 41%, p = 0.804).
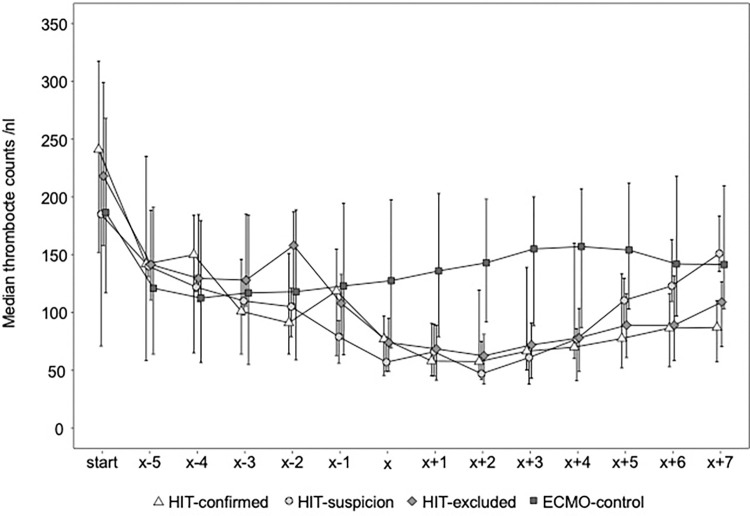
Conclusion: HIT is rare on ECMO, should be suspected, if platelets are decreasing, but seems not to increase mortality if treated promptly.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: ML received lecture honoraria from Fresenius Medical Care. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Prevalence and outcome of heparin-induced thrombocytopenia diagnosed under veno-arterial extracorporeal membrane oxygenation: a retrospective nationwide study.Intensive Care Med. 2018 Sep;44(9):1460-1469. doi: 10.1007/s00134-018-5346-y. Epub 2018 Aug 22. Intensive Care Med. 2018. PMID: 30136139
-
Argatroban versus heparin in patients without heparin-induced thrombocytopenia during venovenous extracorporeal membrane oxygenation: a propensity-score matched study.Crit Care. 2021 Apr 29;25(1):160. doi: 10.1186/s13054-021-03581-x. Crit Care. 2021. PMID: 33910609 Free PMC article.
-
[Application of argatroban in patients receiving extracorporeal membrane oxygenation support: a case-control study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Dec;34(12):1305-1310. doi: 10.3760/cma.j.cn121430-20220701-00621. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36567588 Chinese.
-
Heparin-induced thrombocytopenia complicating extracorporeal membrane oxygenation support in pediatric patients: review of the literature and alternative anticoagulants.Perfusion. 2018 May;33(1_suppl):7-17. doi: 10.1177/0267659118766723. Perfusion. 2018. PMID: 29788841 Review.
-
Heparin-induced thrombocytopenia complicating extracorporeal membrane oxygenation support: Review of the literature and alternative anticoagulants.J Thromb Haemost. 2019 Oct;17(10):1608-1622. doi: 10.1111/jth.14575. Epub 2019 Aug 4. J Thromb Haemost. 2019. PMID: 31313454 Review.
Cited by
-
Anticoagulation and associated complications in veno-arterial extracorporeal membrane oxygenation in adult patients: A systematic review and meta-analysis.Crit Care Resusc. 2024 Nov 26;26(4):332-363. doi: 10.1016/j.ccrj.2024.10.003. eCollection 2024 Dec. Crit Care Resusc. 2024. PMID: 39781486 Free PMC article. Review.
-
Heparin-Induced Thrombocytopenia in Patients Undergoing Venoarterial Extracorporeal Membrane Oxygenation.J Clin Med. 2023 Jan 2;12(1):362. doi: 10.3390/jcm12010362. J Clin Med. 2023. PMID: 36615162 Free PMC article.
-
Heparin-induced thrombocytopenia in extracorporeal membrane oxygenation-supported patients: a systematic review and meta-analysis.Thromb J. 2024 Jun 28;22(1):55. doi: 10.1186/s12959-024-00624-5. Thromb J. 2024. PMID: 38937784 Free PMC article.
References
-
- Protti A, Iapichino GE, Di Nardo M, Panigada M, Gattinoni L. Anticoagulation Management and Antithrombin Supplementation Practice during Veno-venous Extracorporeal Membrane Oxygenation: A Worldwide Survey. Anesthesiology 2019. - PubMed
-
- Greinacher A. Heparin-Induced Thrombocytopenia. N Engl J Med 2015; 373(19):1883–4. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
