

Exploiting the advantages of a wireless seed localization system that differentiates between the seeds: Breast cancer resection following neoadjuvant chemotherapy
- PMID: 35940632
- PMCID: PMC9875611
- DOI: 10.1002/cnr2.1690
Exploiting the advantages of a wireless seed localization system that differentiates between the seeds: Breast cancer resection following neoadjuvant chemotherapy
Abstract
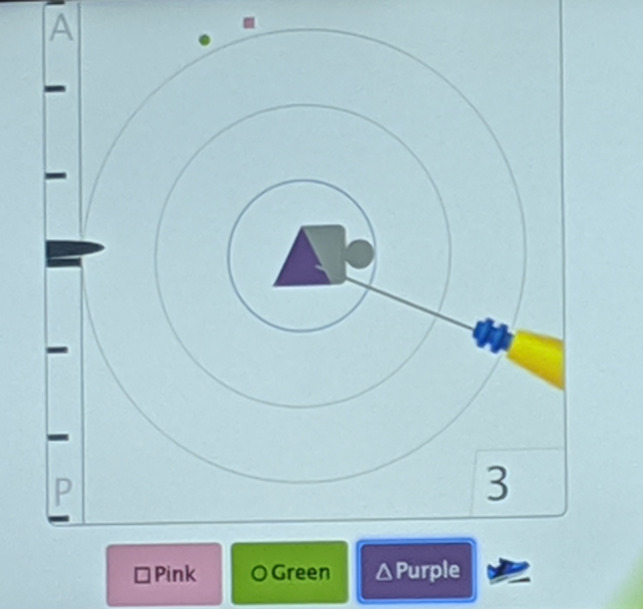
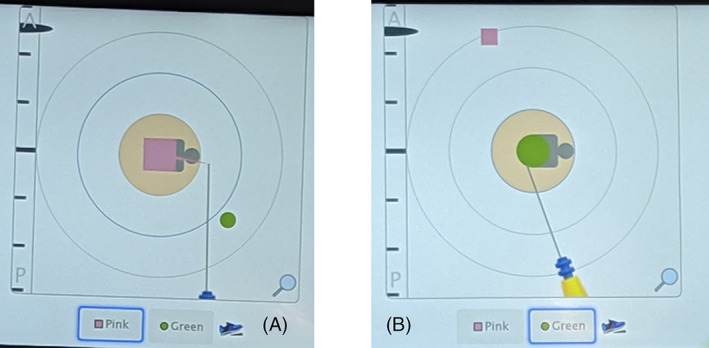
Background: Most wireless localization methods utilize only one means of detection for the surgeon, sufficient to localize a single small breast lesion for excision. Complex cases requiring bracketing of a larger lesion or localization of two or more close lesions can superimpose the signal from separate "seeds" with such methods. The lack of discernment between the localization "seeds" can disorient the surgeon, risking a missed lesion on excision and longer operative times. with the use of neoadjuvant chemotherapy prior to breast surgery, the necessity of localizing both a breast lesion and an axillary lymph node previously biopsied is becoming frequent.
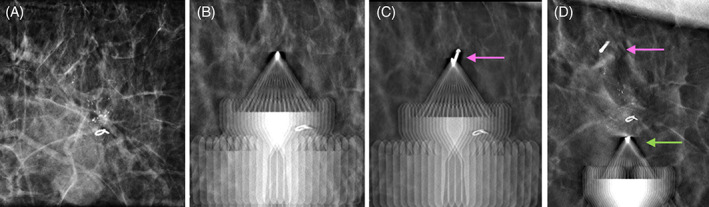
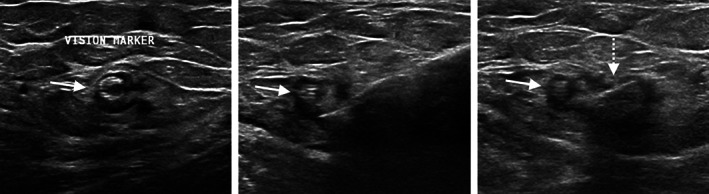
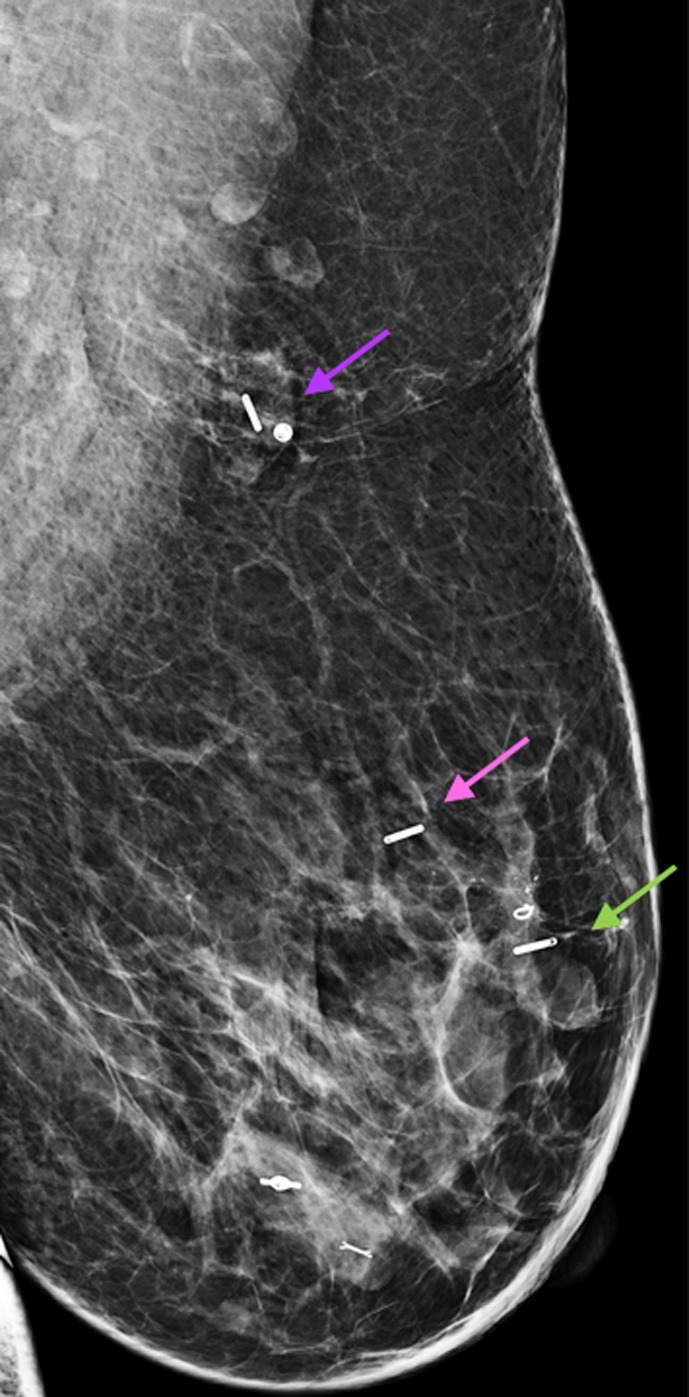
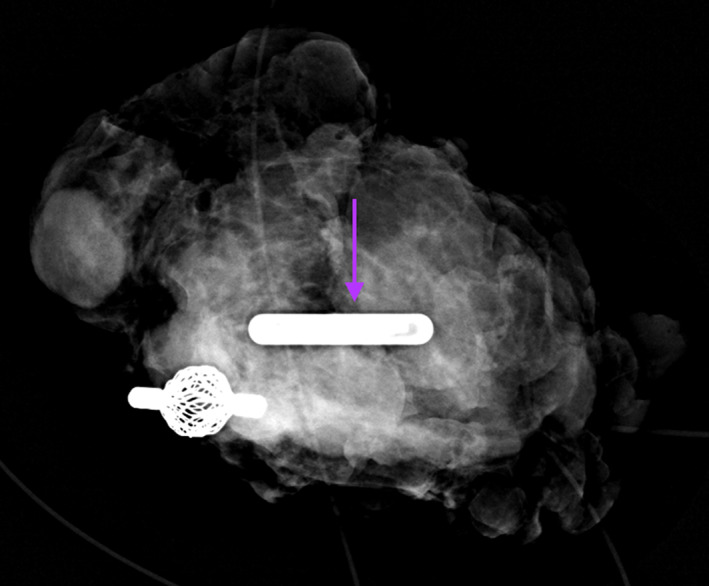
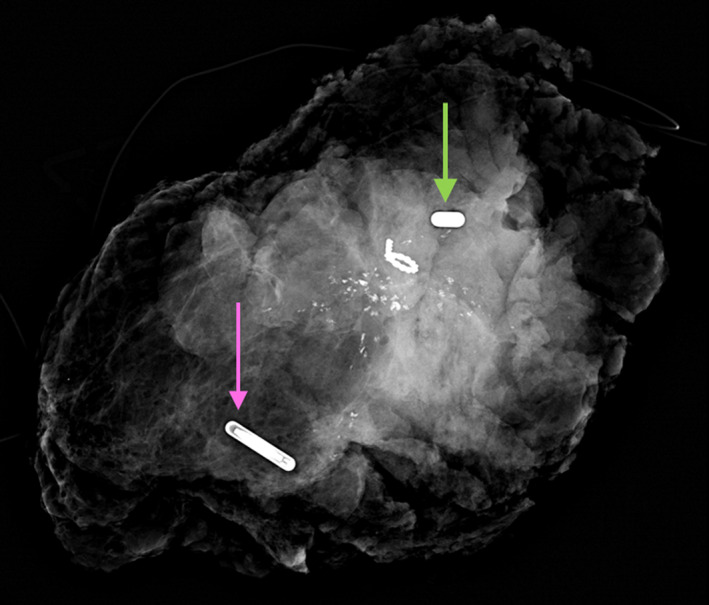
Case: A 44 year-old woman underwent neoadjuvant chmotherapy for a breast cancer the did not express estrogen receptor, progesterone receptor, or HER2 receptor. In establishing the extent of disease, a suspicious ipsilateral lymph node was biopsied and found to contain metastatic disease. She had an excellent response to the chemotherapy, with decreased size of the primary tumor and the previously biopsied lymph node. The patient desired breast conservation. The primary tumor and associated calcifications were bracketed using two different Smartclips™, with a third localizing the lymph node biopsied.
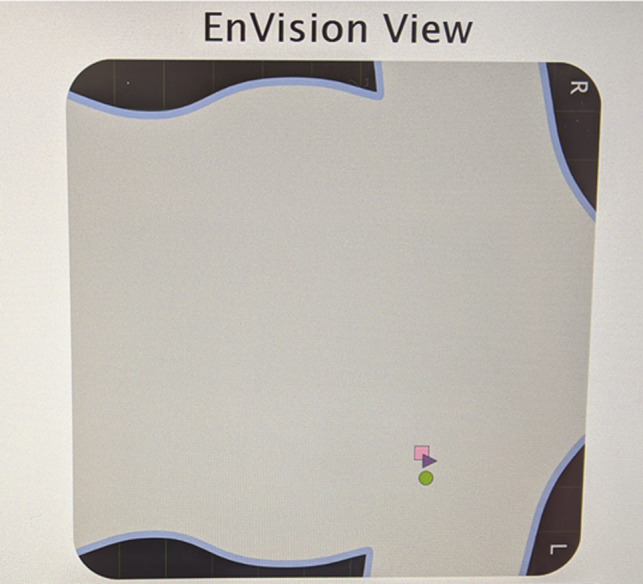
Conclusion: This report illustrates how the use of three SmartClips™, within the EnVisioTM system, allowed for separate tracking of each "seed" throughout a complex surgery in a patient following neoadjuvant chemotherapy. This resulted in successful resection of both the tumor and the tagged lymph node.
Keywords: breast localization; tagged axillary dissection; tagged lymph node; wireless localization.
© 2022 The Authors. Cancer Reports published by Wiley Periodicals LLC.
Conflict of interest statement
Dr. Chantal Reyna recently became a consultant for Elucent Medical. The remaining authors have explicitly stated that there are no conflicts of interest in connection with this article.
Figures

Similar articles
-
Advantages of preoperative localization and surgical resection of metastatic axillary lymph nodes using magnetic seeds after neoadjuvant chemotherapy in breast cancer.Surg Oncol. 2021 Mar;36:28-33. doi: 10.1016/j.suronc.2020.11.013. Epub 2020 Nov 23. Surg Oncol. 2021. PMID: 33285433
-
Targeted axillary dissection with preoperative tattooing of biopsied positive axillary lymph nodes in breast cancer.Neoplasma. 2020 Nov;67(6):1329-1334. doi: 10.4149/neo_2020_191228N1344. Epub 2020 Aug 4. Neoplasma. 2020. PMID: 32749847
-
SAVI SCOUT® localization of metastatic axillary lymph node prior to neoadjuvant chemotherapy for targeted axillary dissection: a pilot study.Breast Cancer Res Treat. 2022 Jan;191(1):107-114. doi: 10.1007/s10549-021-06416-z. Epub 2021 Oct 15. Breast Cancer Res Treat. 2022. PMID: 34652548 Clinical Trial.
-
Intraoperative sentinel lymph node evaluation in patients with node-positive breast cancer status post neoadjuvant systemic therapy - An institutional experience.Ann Diagn Pathol. 2022 Oct;60:152012. doi: 10.1016/j.anndiagpath.2022.152012. Epub 2022 Jul 22. Ann Diagn Pathol. 2022. PMID: 35908331 Review.
-
The problem of axillary staging in breast cancer after neoadjuvant chemotherapy. Role of targeted axillary dissection and types of lymph node markers.Cir Esp (Engl Ed). 2020 Nov;98(9):510-515. doi: 10.1016/j.ciresp.2020.03.012. Epub 2020 May 6. Cir Esp (Engl Ed). 2020. PMID: 32386728 English, Spanish.
Cited by
-
Innovations in the localization techniques for non-palpable breast lesions: Make invisible visible.Breast. 2025 Jun;81:104430. doi: 10.1016/j.breast.2025.104430. Epub 2025 Feb 26. Breast. 2025. PMID: 40056722 Free PMC article. Review.
-
Localization Techniques for Non-Palpable Breast Lesions: Current Status, Knowledge Gaps, and Rationale for the MELODY Study (EUBREAST-4/iBRA-NET, NCT 05559411).Cancers (Basel). 2023 Feb 12;15(4):1173. doi: 10.3390/cancers15041173. Cancers (Basel). 2023. PMID: 36831516 Free PMC article. Review.
-
Resection Ratios and Tumor Eccentricity in Breast-Conserving Surgery Specimens for Surgical Accuracy Assessment.Cancers (Basel). 2024 May 9;16(10):1813. doi: 10.3390/cancers16101813. Cancers (Basel). 2024. PMID: 38791892 Free PMC article.
References
-
- Hasselgren PO, Hummel RP, Georgian‐Smith D, Fieler M. Breast biopsy with needle localization: accuracy of specimen X‐ray and management of missed lesions. Surgery. 1993;114(4):836‐840. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
