

Ambulances Required to Relieve Overcapacity Hospitals: A Novel Measure of Hospital Strain During the COVID-19 Pandemic in the United States
- PMID: 35940995
- PMCID: PMC9356618
- DOI: 10.1016/j.annemergmed.2022.05.036
Ambulances Required to Relieve Overcapacity Hospitals: A Novel Measure of Hospital Strain During the COVID-19 Pandemic in the United States
Abstract
Study objective: One in 4 deaths from COVID-19 has been attributed to hospital crowding. We simulated how many ambulances would be required to rebalance hospital load through systematic interhospital transfers. We assessed the potential feasibility of such a strategy and explored whether transfer requirement was a helpful measure and visualization of regional hospital crowding during COVID-19 surges.
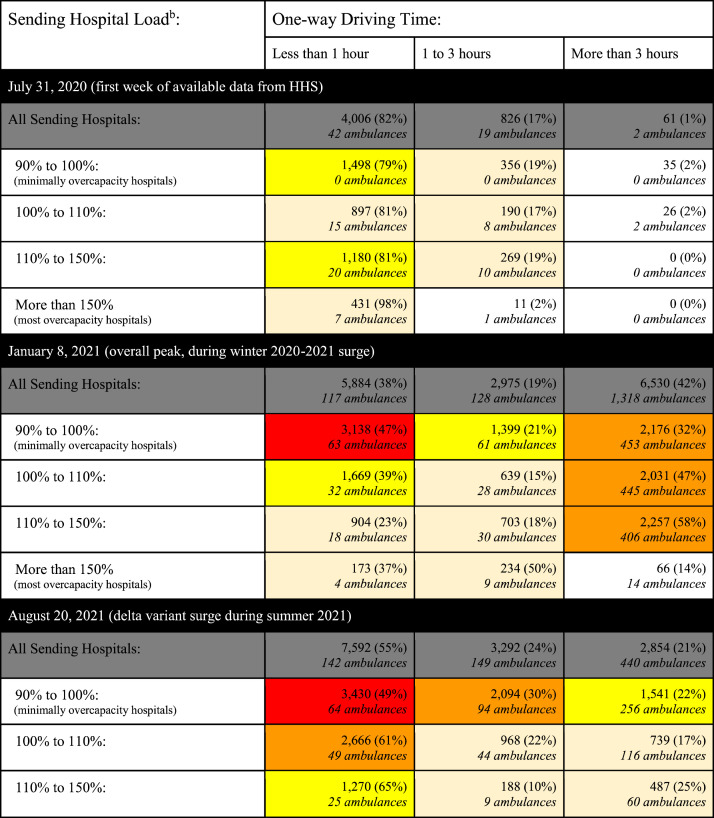
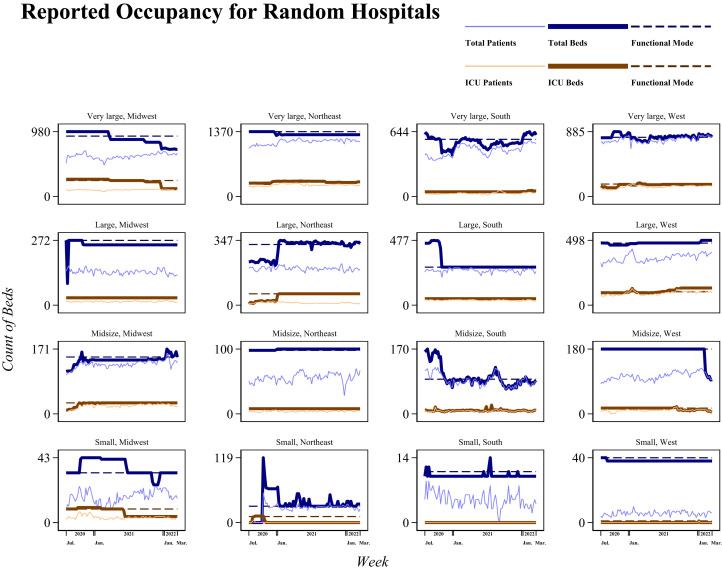
Methods: Using data from the United States hospitals reporting occupancy to the Department of Health and Human Services from July 2020 to March 2022 and road network driving times, we estimated the number of ambulances required weekly to relieve overcapacity hospitals.
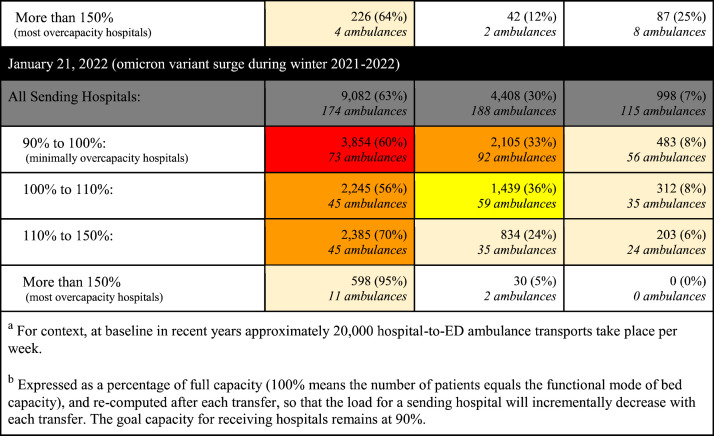
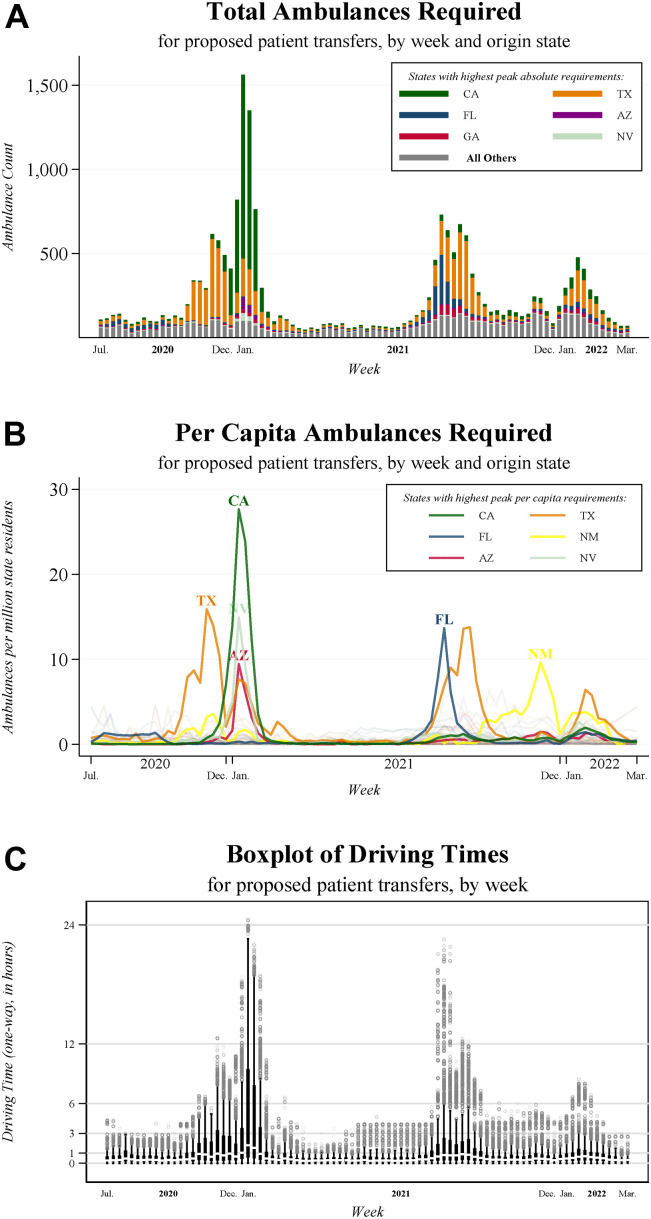
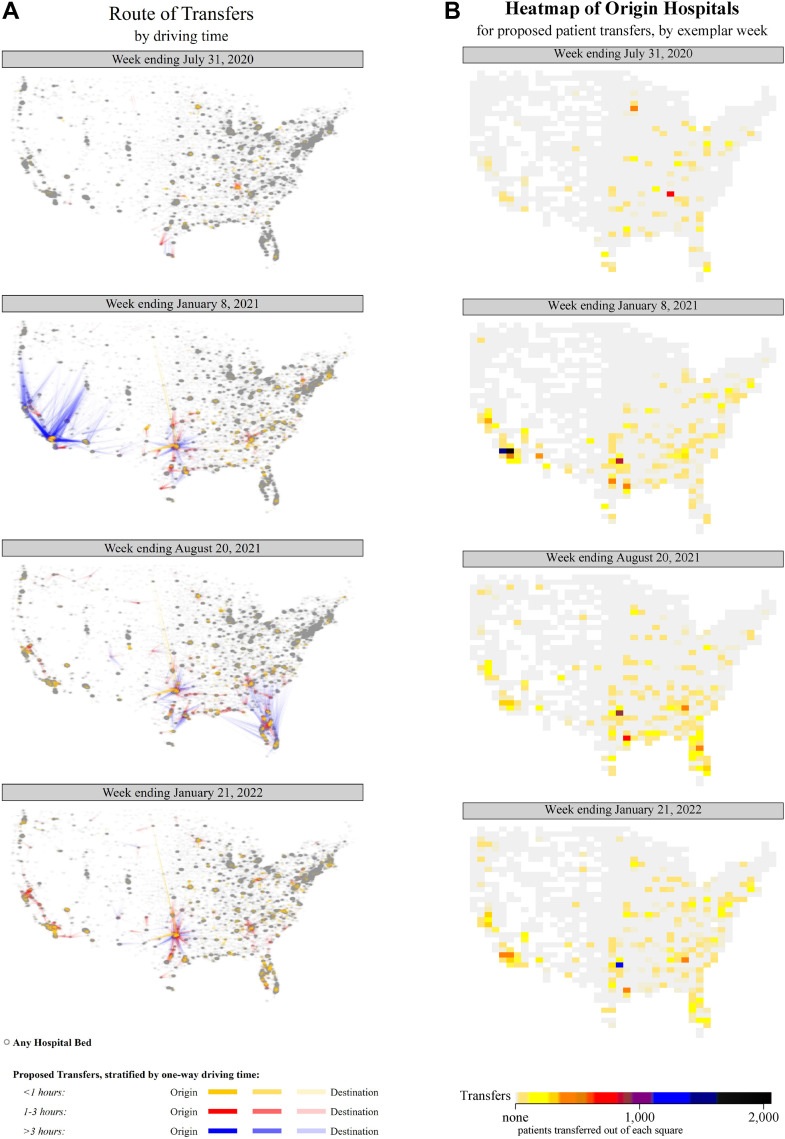
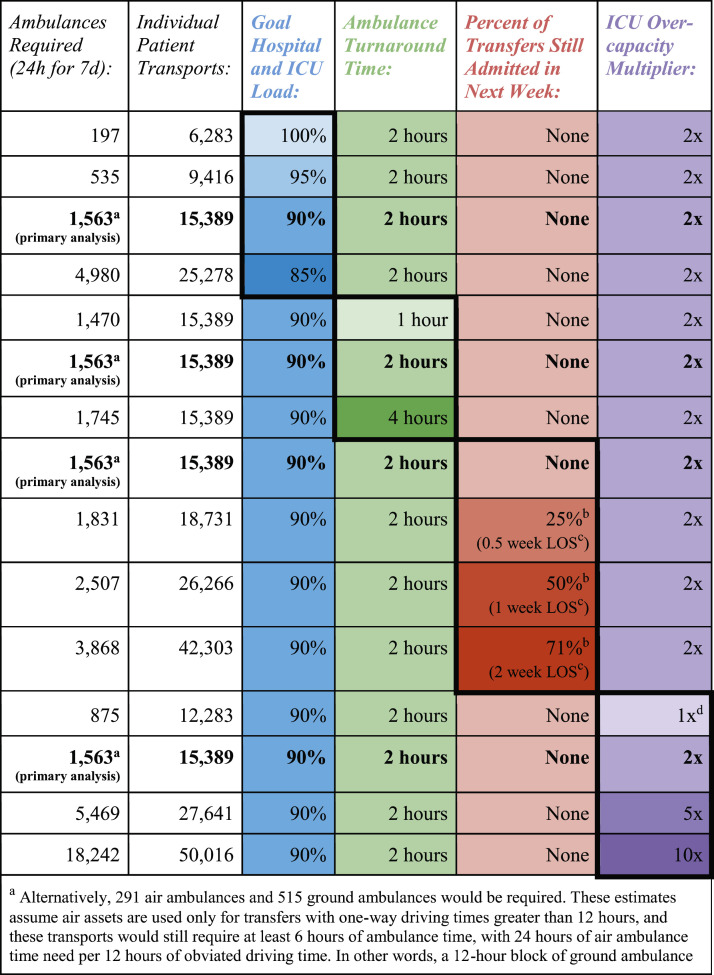
Results: During the peak week, which ended on January 8, 2021, approximately 1,563 ambulances would be needed for 15,389 simulated patient transports, of which 6,530 (42%) transports involved a 1-way driving time of more than 3 hours. Transfer demands were dramatically lower during most other weeks, with the median week requiring only 134 ambulances (interquartile range, 84 to 295) and involving only 116 transports with 1-way driving times above 3 hours (interquartile range, 4 to 548). On average, receiving hospitals were larger and located in more rural areas than sending hospitals.
Conclusion: This simulation demonstrated that for most weeks during the pandemic, ambulance availability and bed capacity were unlikely to have been the main impediments to rebalancing hospital loads. Our metric provided an immediately available and much more complete measure of hospital system strain than counts of hospital admissions alone.
Copyright © 2022 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Response to "Ambulances Required to Relieve Overcapacity Hospitals: A Novel Measure of Hospital Strain during the COVID-19 Pandemic in the United States".Ann Emerg Med. 2023 May;81(5):644-645. doi: 10.1016/j.annemergmed.2022.12.030. Ann Emerg Med. 2023. PMID: 37085207 Free PMC article. No abstract available.
