

Unified classification and risk-stratification in Acute Myeloid Leukemia
- PMID: 35941135
- PMCID: PMC9360033
- DOI: 10.1038/s41467-022-32103-8
Unified classification and risk-stratification in Acute Myeloid Leukemia
Abstract
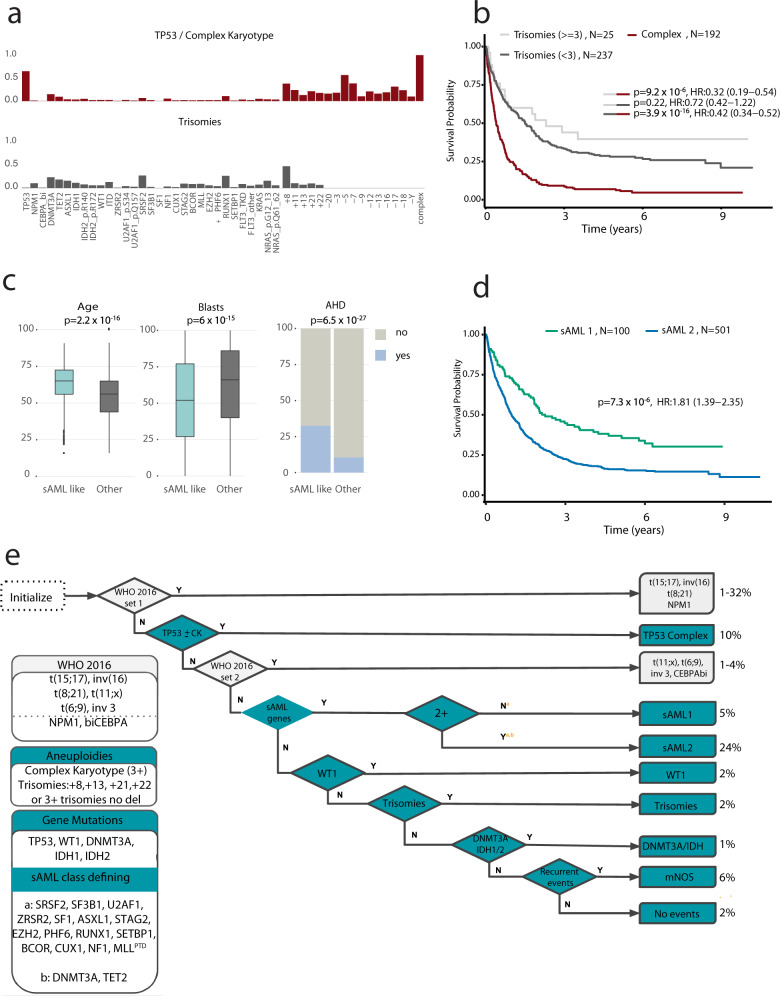
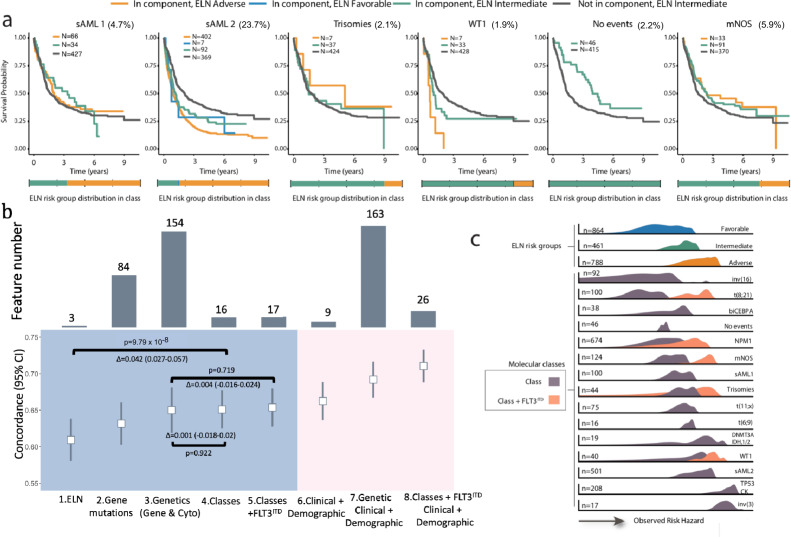
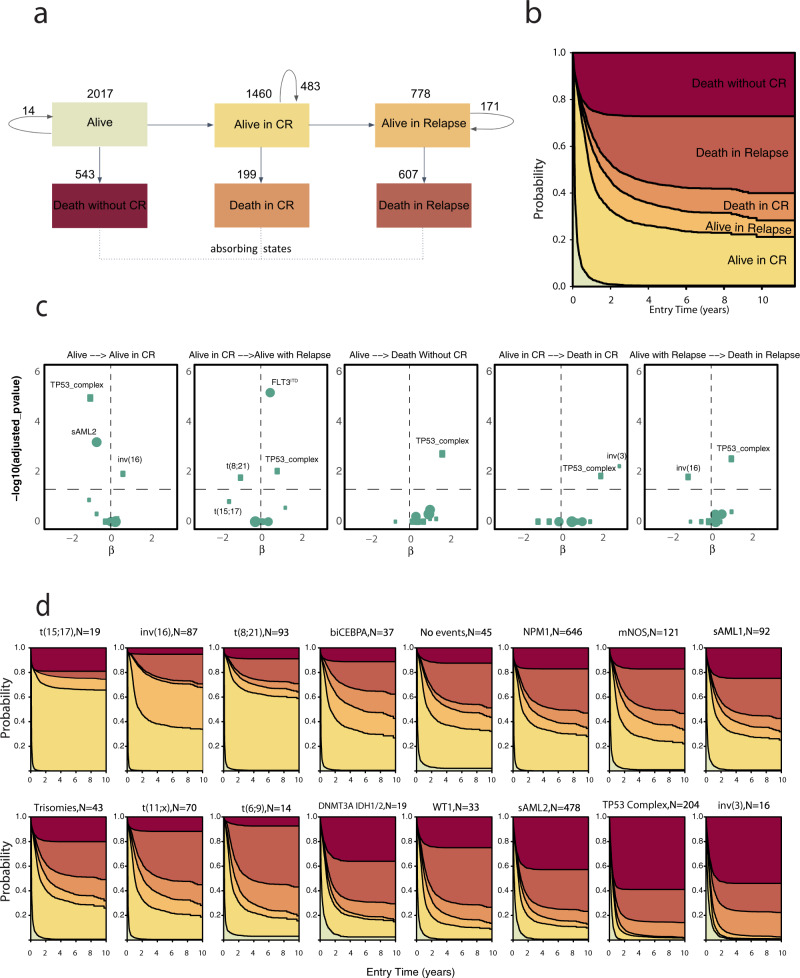
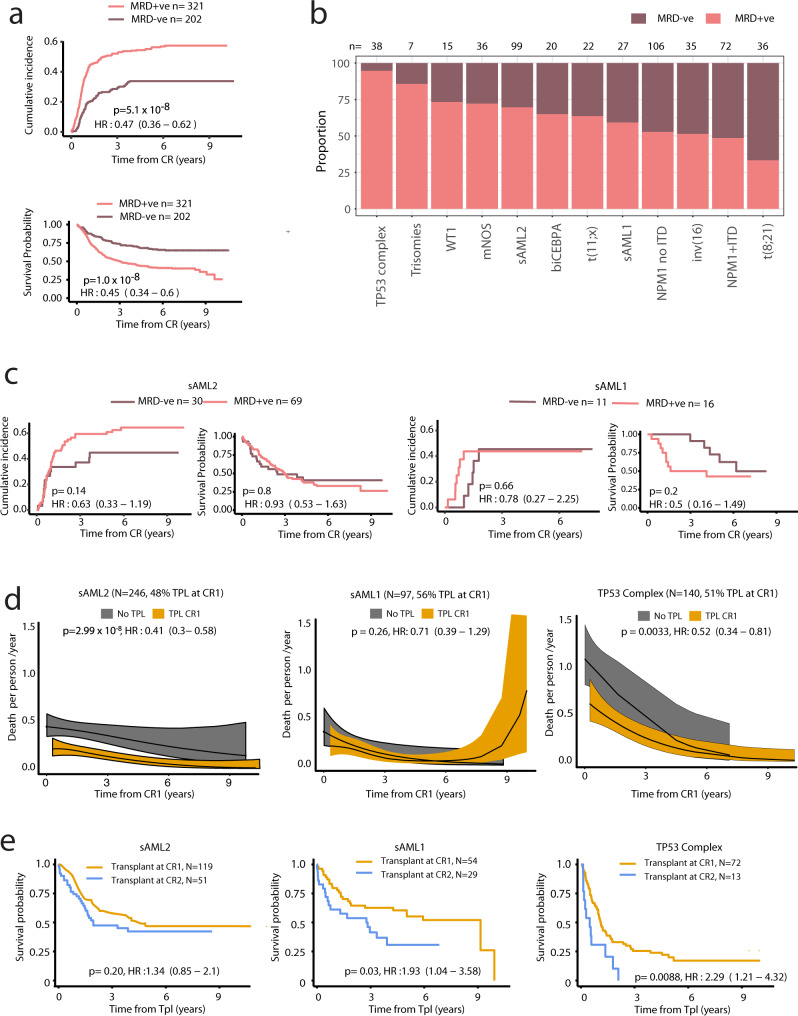
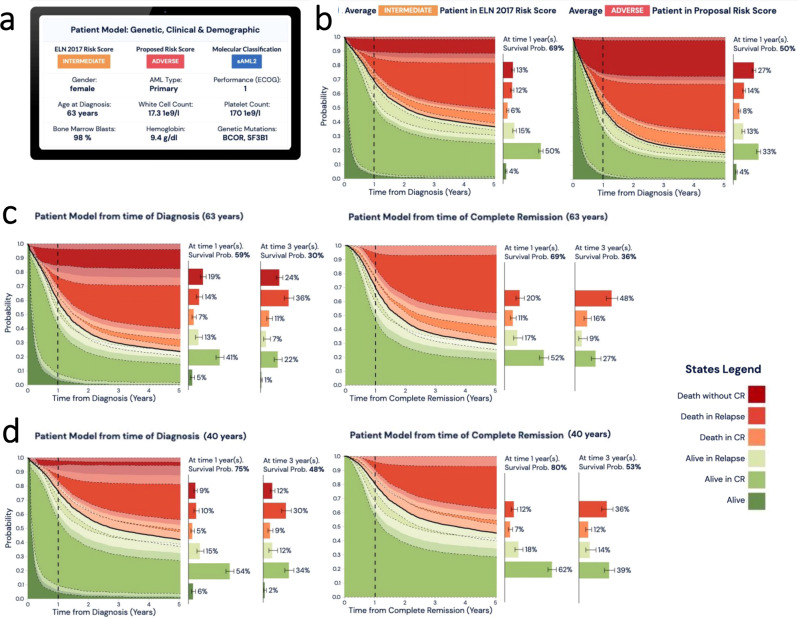
Clinical recommendations for Acute Myeloid Leukemia (AML) classification and risk-stratification remain heavily reliant on cytogenetic findings at diagnosis, which are present in <50% of patients. Using comprehensive molecular profiling data from 3,653 patients we characterize and validate 16 molecular classes describing 100% of AML patients. Each class represents diverse biological AML subgroups, and is associated with distinct clinical presentation, likelihood of response to induction chemotherapy, risk of relapse and death over time. Secondary AML-2, emerges as the second largest class (24%), associates with high-risk disease, poor prognosis irrespective of flow Minimal Residual Disease (MRD) negativity, and derives significant benefit from transplantation. Guided by class membership we derive a 3-tier risk-stratification score that re-stratifies 26% of patients as compared to standard of care. This results in a unified framework for disease classification and risk-stratification in AML that relies on information from cytogenetics and 32 genes. Last, we develop an open-access patient-tailored clinical decision support tool.
© 2022. The Author(s).
Conflict of interest statement
E.P. is a founder, equity holder and has a fiduciary role in Isabl, a cancer whole genome sequencing analytics company. The remaining authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
- MC_PC_17230/MRC_/Medical Research Council/United Kingdom
- BRC-1215-20014/DH_/Department of Health/United Kingdom
- 203151/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MR-R009708-1/MRC_/Medical Research Council/United Kingdom
- C18680/A25508/CRUK_/Cancer Research UK/United Kingdom
- P30 CA008748/CA/NCI NIH HHS/United States
- 25508/CRUK_/Cancer Research UK/United Kingdom
- 25643/CRUK_/Cancer Research UK/United Kingdom
- MR/R009708/1/MRC_/Medical Research Council/United Kingdom
- C49940/A25117/CRUK_/Cancer Research UK/United Kingdom
- 205254/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- 29806/CRUK_/Cancer Research UK/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- 25350/CRUK_/Cancer Research UK/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
